



Articles - Year 1997 - Volume 12 -
Esthetic Correction of Pectus Excavatum
Pectus excavatum: Correção Cirúrgica Estética
ABSTRACT
Pectus exeavatum is the most common deformity of the chest wall. The scope ofthe technique described is to resolve the esthetic part ofthis pathology. Two cases are used to illustrate this work which employs adipose glandularflaps advanced toward the mid-portion ofthe thorax. A silicone prosthesis was inserted in the female patient. Ifcorrectly indicatedandexecuted, this minimally invasive technique achieves satisfactofY esthetic results with lower post-operative morbidity.
Keywords: Pectus Excavatum, Funnel Chest, Thoracic Deformity
RESUMO
O Pectus excavatum é a mais comum das deformidades da parede torácica. Inúmeras técnicas cirúrgicas foram propostas para a correção dos diversos graus dessa patologia. A técnica descrita tem por objetivo a correção do Pectus excavatum como deformidade puramente estética. Os autores descrevem dois casos de retalhos adiposo-glandulares em avanço para a linha médio-esternal, sendo que na paciente do sexo feminino foi associada inclusão de prótese de silicone. Observa-se que, quando bem indicada e executada, essa técnica pouco invasiva oferece resultados estéticos satisfatórios associados a menor morbidade pós-operatória.
Palavras-chave: Pectus excavatum, Peito em Funil, Deformidade Torácica
Pectus excavatum is the most common chest wall deformity(6). The pathology presents with an acute posterior curvature of the chest, extending from the manubrium to the xiphoid process, and is deeper on the distal portion.
Sometimes, associated defects may be present, i.e., protruding abdomen, kyphoscoliosis, hypomastia and rarely cardiorespiratory pathologies(1).
Various theories have been proposed to explain this defect, among them the intrauterine position of the ferus, rickets, presence of a substernal ligament which would promote depression of the sternum, retraction of the central tendon of the diaphragm, congenital aplasia of tbe sternum, congenitally short rectus muscles, mediastinal tumor and hereditary syphilis(1). However, the most acceptable explanation is that there might be an unproportional growth ofthe rib cartilages and consequently retroposition of the sternum. The latter is termed Pectus excavatum, or if the sternum is positioned anteriorly, the result is Pectus carinatum(3).
Occasionally, the sternal retroposition may affect the cardiae and/or pulmonary dynamics. A systolic murmur can be heard in these patients and a chest X ray reveals heart displacement. The ECG may demonstrate axis deviation, abnormal P waves and conduction disturbances. In spite of these findings, the majority of patients are asymptomatic and without functional impairment(11).
The first report of this pathology is attributed to Bauhinus(2)in 1594. In 1913, Sauerbruch(12) accomplished the first successful corrective surgery. Ochsner and DeBakey(8), in 1939, presented a classical study, on the surgical treatment of this pathology. Brnwn and Raviteh(10), subsequently defined the basic principles for correction of Pectus excavatum. Since then, various modifications requiring costochondral dissection and mobilization of the sternum have been described. In 1965, Murray(7) reported the insertion ofa silicone implant for correction of the defect, a technique utilized with some modifications, until the present time. The aim of the procedure described is to correct the esthetic element of the pathology and two cases will be used to illustrate this.
Material and Methods
This study was conducted in 1995, in the "Centro Cientifico Brasileiro de Cirurgia Plastica", Santos-Sao Paulo. Two patients underwent surgery: a white, 18 years old male with only a cosmetic defect, without cardiorespiratory symptoms and with a moderate amount of adipose-glandular tissue in the chest wall. The other patient was a white, 31 years old female, without cardiorespiratory problems, with sternal depression associated with lateralization of the breasts, and on profile, showed the areola corresponding to the highest point of the sternum. Because of her body image, this patientalso presented with severe psychological changes.
Operative Technique
The technique employed adipose-glandular flaps together with a silicone prosthesis in the female patient.
In this patient, an incision about 0.7 em long was made in the projection of the submammary fold followed by wide undermining ofthe supra-aponeurotic plane which also included the excavated portion of the sternum.
Then by undermining the subcutaneous layer, an adipose-glandular flap was fashioned from the internal part of each breast (internal pedicle) (Fig. 1). These flaps were rotated medially and sutured to the excavated portion of the chest and the rest of each breast was turned to close the dead space left by the flap rotation (Fig. 2). After meticulous hemostasis, the silicone prosthesis were placed and the skin sutured (2-0 mononylon intradermic suture). Suction drains, exteriorized by a stab wound were employed and maintained until the volume was reduced to 30 ml/ day, corresponding to five days.
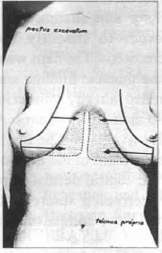
Fig. 1 - Adipose-glandular flap.

Fig. 2 - Rotation of the flaps.
A 0.8 em long midsternal fusiform incision was made in the male patient. This incision was used to attach the adipose-glandular and dermo-adipose flaps (Fig. 3).

Fig. 3 - Midsternal fusiform incision.
Wide supra-aponeurotic undermining was also accomplished, limited by: the anterior axillary line, projection of the mammary fold and projection of the second rib.
The adipose-glandular flaps were fashioned bi laterally (Fig. 4) and as an auxilliary procedure, an incision was made in the areolar-mammillary unit (transareolarmammillary incision) in order to simplify the undermining and review the hemostasis.

Fig. 4 - Adipose-glandular tissue.
The flaps were advanced in the direction of the thoracic midline and fixed at the base ofthe fusiform flap (already without its epidermis), with interrupted 2-0 mononylon sutures. A suction drain was maintained for five days. The finalstep was the tension-free advancement of the dermoadipose flaps in direction to the central dermal flap, with a dermal-dermal type interrupted suture (2-0 mononylon), thereby, permitting the compartments to remain isolated.
LDressings in both patients were accomplished with bandage gauze and #28 foam rubber, placed on the wound area, maintaining light pressure for 30 days; antibiotic therapy begun intraoperatively was maintained until the seventh post-operative day, when the skin sutures were removed.
Results
This technique enabled the patient to recover quickly with low p.o. morbidity, the mean hospital stay was reduced (only one day). In both patients the drains were removed on the fifth p.o. day. No infections or dehiscenses occurred nor did seromas or hematomas forn1.
The scars wereestheticallypleasing, which contributed much to increase the patients satisfaction with their body image (Figs. 5,6,7,8).
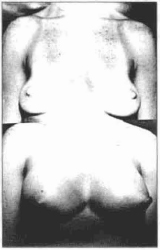
Fig. 5 - Female patient; pre and post-operative frontal aspect.

Fig. 6 - Female patient; pre and post-operative 3/4 left profile.
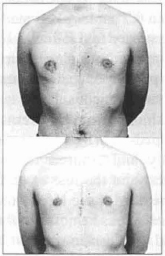
Fig. 7 - Male patient; pre and post-operative fromal aspect.
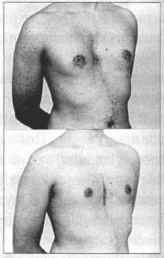
Fig. 8 - Male patient; pre and post-operative 3/4 right profile.
Discussion
According to the literature, the etiology of Pectus excavatum is secondary to an excessive growth of the ribs dislocating the sternum to accomodate them(3).
This defect is usually present at birth and progresses with the child's growth. After adolescence, it is characteristically associated with lombodorsal scoliosis, round shoulders and protruding abdomen(1).
Regarding surgical indication: patients with cardiac changes, dyspnea on exercise, palpitations and chest pains related to pectus excavatum, are candidates for costochondral reconstruction.
Subjects with esthetic alterations without cardiorespiratory involvement, are benefitted by this technique, since a thoracic prosthesis is not used, they do not present complications such as displacements, visualization of the prosthesis(3) profile or extrusion.
We would like to point out that breast prosthesis placed at a second 1 stage would be better indicated because the adipose-glandular or dermo-adipose flaps occasionally present various degrees ofischemia and the prosthesis placed at the same surgical stage may lead to compression and ischemia of the flaps.
Conclusion
The technique reported achieved satisfactory results, it is accomplished in a single stage, pennits a rapid recovery and without large scars.
Since the most common indication for Pectus excavatum is esthetic(5), it is mandatory that we employ the simplest and safest procedure, a condition fully met by this technique.
References
1. ASTON J.S., PICKRELL L.K. - Chest wall rcconstruction. In: CONVERSE, J. M. Reconstructive Plastic Surgery. Volume VIl. 2nd. Edition. Philadelphia, W.E. Saunders, 1977, p. 3633-45.
2. BAUHINUS J. Apoud - MARKS M.W., ARGENTA L.C., LEE D.C. Silicone implant correction of Pectus Excavatum: indication and refinement in technique. Plast Reconstr. Surg. 74:52-8, 1984.
3. EHRE HAT T.L., ROSSI N.P., LAURENCE M.S. - Development chest wall defects. Ann. Thorac. Surg., 2: 384, 1966.
4. FUGIMO T., HARASHIMA T., AOYGE F. Reconstruction for aplasia of the breast and pectoral region by microvascular transfer of a free flap from the buttock. Plast. Reconstr.Surg., 56: J78, 1975.
5. HUMPHREYS G.H., JARETZKJ A. - Operative correction ofPectus excavatum.J. Pedial. Surg., 9: 899, 1974.
6. MARKS M.W., ARGE TA L.C., LEE D. C.Silicone implant correction ofPectusExcavatum: Indication and rcfmcmcnt in technique. Plast. Reconstr. Surg. 1:52 - 8, 1984.
7. MURRAY J.F.Apoud-MARKSM.W.,ARGENTA L.c., LEE D.C. - Silicone implant correction of Pectus excavatum: Indication and refinement in techcnique. Plasl. Reconstr. Surg., 74: 52 - 8, 1984.
8. OSCHNER A., DEBAKEY M. - Chonechondrosternun: Report ofa case and review of the literature. J. Thorac. Surg., 8: 469, 1939.
9. PIERRE M. L., JOUGLARD J.P. - Treatment of wlilateral congenital hypoplasia or absence ofthe breast. Plast Reconstr. Surg., 56: 146, 1975.
10. RAVlTCH M.M. - The operative treatment ofPectus excavaturn. Ann. Surg., 129: 429, 1949.
11. REUSCH C.S. - Hemodynamic studies in Pectus excavaturn. Circulation, 24: 1143, 1961.
12. SAUERBRUCH D.F. - Apoud - MARKS M.W., ARGENTA L.c., LEE D.C. Silicone implant correction of Pectus excavatwn: indication and refinement in technique.Plast. Reconstr. Surg., 74: 52-4, 1984.
I - Clillical Director "Celltro Cielltijico Brasileiro de Cimrgia Plasfica Deportmellt o/Plasfic Surgery. Universidade Santa Cecilia dos Bandeirantes (USCB)
II - Member Braoilian Society of Plastic Surgery; Assistant, Plastic Surgery Service, USCB
III - Assislallt Physiciall. Plastic Surgery Service, USCB
IV - Resident, Plastic Surgery Service, USCB
ADDRESS FOR CORRESPONDENCE
Centro Cientifico Brasileiro de Cirurgia Plastica
Av. Ana Costa, 120 - Vila Mathias - Santos
CEP 11060-000 - Sao Paulo - Brazil
Tel: (0132) 34-1235 / Fax: (0132) 33-6028
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket