



Case Report - Year 2022 - Volume 37 -
Use of retroauricular tubular flap for ear helix and ear lobe reconstruction
Uso do retalho tubular retroauricular para reconstrução da hélice e lóbulo da orelha
Renato da Silva Freitas2 ; Caio Munaretto Giacomazzo1,*; Silvia Helena Mandu2; Maria Cecilia Closs Ono2; Alfredo Duarte da Benjamin Silva2
; Caio Munaretto Giacomazzo1,*; Silvia Helena Mandu2; Maria Cecilia Closs Ono2; Alfredo Duarte da Benjamin Silva2
ABSTRACT
Ear defects are frequent and result of many etiologies, even though ear reconstruction remains a challenge in plastic reconstructive surgery due to anatomy and local tissue paucity. Despite being rarely used, the tubular retroauricular flap presents as an alternative for helix and lobule reconstruction. In this article, the authors describe the operative technique and report a case in which it was used. Also, plastic surgeons and laypeople rated the operative results of four cases of ear reconstructions using the tubular retroauricular flap. The final esthetic result was rated as good or excellent by 35% of laypeople and 50% of plastic surgeons, whereas the operative result was rated as good or excellent by 70% of laypeople and 80% of plastic surgeons. Thereby the findings and authors' experience, we can recommend the tubular retroauricular flap technique for reconstructing ear helix border defects.
Keywords: Ear; Ear external; Reconstructive surgical procedures; Surgical flaps; Congenital abnormalities.
RESUMO
Defeitos de orelha são frequentes e de etiologias diversas. Ainda assim, a reconstrução de orelha permanece um desafio dentro da cirurgia plástica reconstrutiva, principalmente devido a anatomia e a escassez de tecido local. Embora pouco utilizado, o retalho tubular retroauricular se apresenta como alternativa para reconstrução da hélice e lóbulo. No presente estudo os autores descrevem a técnica operatória, bem como relatam um caso em que foi utilizado. Realizou-se uma avaliação do resultado operatório de quatro casos de reconstrução de orelha utilizando o retalho tubular retroauricular, através de questionários encaminhados para avaliadores leigos e cirurgiões plásticos. O resultado estético final foi classificado como bom ou excelente por 35% dos avaliadores leigos e 50% dos cirurgiões plásticos. Já o resultado operatório foi avaliado como bom ou excelente por 70% dos leigos e 80% dos cirurgiões plásticos. Os resultados permitem concluir que a técnica do retalho tubular retroauricular para reconstrução de defeitos da borda de hélice pode ser indicada, com resultados satisfatórios.
Palavras-chave: Orelha; Orelha externa; Procedimentos cirúrgicos reconstrutivos; Retalhos cirúrgicos; Anormalidades congênitas
INTRODUCTION
Descriptions of earlobe reconstruction by Sushruta date from approximately the 6th century BC. Much progress has been made in ear reconstruction, especially in the 20th century. However, the morphological variability of the defects, associated with the few options for skin coverage, makes ear reconstruction a challenge for plastic surgery1.
Ear defects may involve the skin of the anterior region, the cartilage, and/or the skin of the retroauricular region. Therefore, the reconstruction process must be based on replacing lost tissues. The scarcity of skin tissue in the area makes these cases a challenge in reconstruction.
Ear defects with partial loss of the helix can occur due to trauma, bites, neoplasm resections and burns. The different etiologies make these imperfections frequent; however, the local anatomy makes these irregularities difficult to reconstruct. The various techniques described in the literature corroborate the inexistence of a definitive technique2,3.
OBJECTIVE
Analysis of the final aesthetic results of a tubular flap for the reconstruction of ear helix defects through pre- and post-operative photos evaluated by plastic surgeons and laypersons.
METHODS
This is a retrospective, observational study of six patients who underwent ear reconstruction with a tubular flap at CAIF - Centro de Atendimento Integral ao Fissurado Lábio-Palatal, at Hospital de Clínicas do Paraná and at a private service, in Curitiba-PR, during the period from 2005 to 2016, operated by the same surgeon.
During 11 years, six patients underwent ear reconstruction using the tubular flap technique. Five patients were female, and one male; the mean age was 53.5 years (22 - 62). The etiology of the defects was divided into three categories: auriculocondylar syndrome - 2, human bite - 1, and traumatic avulsion - 3. middle and lobe in the two remaining ears. No patient was reoperated, and all showed satisfaction with the aesthetic improvement.
Surgical technique
After measuring the defect, the bipedicled flap was drawn on the skin of the mastoid region, with the anterior margin adjacent to the cephaloauricular sulcus. To the length of the flap, 0.5 cm must be added at each end due to the shrinkage of the fabric during transfer. The width is around 1.5 to 2.0 cm and is dependent on the width of the helix defect to be reconstructed. As for depth, the flap was elevated to the subcutaneous tissue level, taking care to preserve the subdermal plexus. The flap is sutured at its anterior edge to the anterior skin of the helix and the posterior edge of the flap to the skin of the retroauricular region. The donor site is closed primarily by advancing the mastoid skin. In this way, the ear is adhered to the mastoid region.
In the second surgical procedure, after at least three weeks, the cephalic pedicle of the tubular flap is released, and the upper margins of the defect are minimally trimmed at a right angle to avoid notches. The donor site has primary closure again.
For the third and final surgical stage, after approximately 14 days, the caudal portion of the tube is disinserted and sutured at right angles to the lower edge of the helix, which is reopened along its length to allow its insertion into the defect.
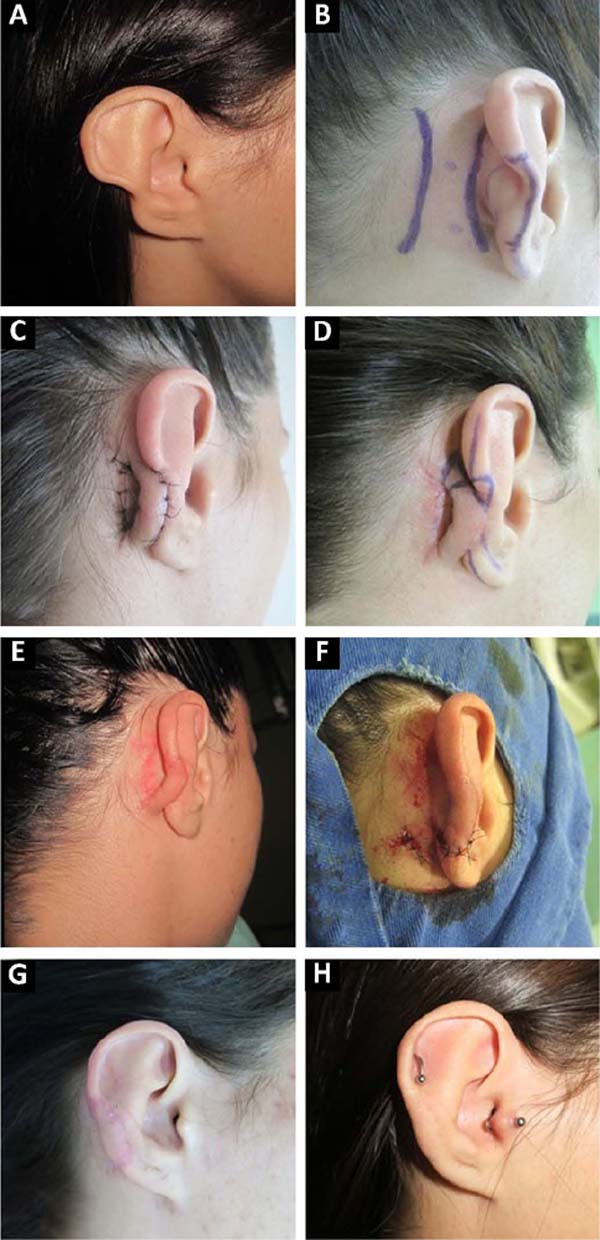
CASE REPORT
Female patient, 19 years old, with auriculocondylar syndrome, presenting bilateral partial helix deformity (Figure 1A). The right ear underwent reconstruction of the defect using the retroauricular tubular flap technique in three surgical stages, as described in this study (Figure 1B-F). Good early and late post-operative aesthetic results (Figure 1G-H).

METHODS
The study included 20 plastic surgeons and 20 laypersons, who evaluated four cases of ears reconstructed using the retroauricular tubular flap technique. The etiology of the defects was trauma (Ears 1 and 2) and auriculo-condylar syndrome (Ears 3 and 4). The evaluation was conducted through two questions and preoperative and post-operative photos with up to 24 months of follow-up. Each participant evaluated only one case, so each ear was evaluated by five surgeons and five laypersons.
The following questions were asked:
Question 1: Evaluate this ear (showing only the post-operative photograph);
Question 2: Evaluate this result (simultaneously displaying the photographs pre- and post-operatively).
Responses were presented on a visual scale, from 1 to 4, with faces (similar to the visual analytical scale for pain), with 1- Bad; 2- Regular; 3- Good; 4- Excellent. The results were compiled and presented through their medians, minimum and maximum values.
RESULTS
The individual scores given by the plastic surgeons and lay participants were detailed in Table 1.
| Evaluator | Question 1 | Question 2 |
|---|---|---|
| Ear 1 | ||
| Surgeon 1 | 3 | 4 |
| Surgeon 2 | 2 | 3 |
| Surgeon 3 | 2 | 2 |
| Surgeon 4 | 2 | 2 |
| Surgeon 5 | 2 | 3 |
| Layman 1 | 2 | 3 |
| Layman 2 | 2 | 2 |
| Layman 3 | 2 | 2 |
| Layman 4 | 3 | 3 |
| Layman 5 | 2 | 3 |
| Ear 2 | ||
| Surgeon 6 | 4 | 4 |
| Surgeon 7 | 1 | 4 |
| Surgeon 8 | 2 | 3 |
| Surgeon 9 | 2 | 3 |
| Surgeon 10 | 2 | 2 |
| Layman 6 | 1 | 3 |
| Layman 7 | 2 | 2 |
| Layman 8 | 1 | 2 |
| Layman 9 | 2 | 2 |
| Layman 10 | 2 | 3 |
| Ear 3 | ||
| Surgeon 11 | 4 | 4 |
| Surgeon 12 | 3 | 4 |
| Surgeon 13 | 3 | 4 |
| Surgeon 14 | 3 | 3 |
| Surgeon 15 | 3 | 3 |
| Layman 11 | 2 | 2 |
| Layman 12 | 2 | 4 |
| Layman 13 | 4 | 4 |
| Layman 14 | 3 | 4 |
| Layman 15 | 4 | 4 |
| Ear 4 | ||
| Surgeon 16 | 2 | 3 |
| Surgeon 17 | 3 | 4 |
| Surgeon 18 | 3 | 4 |
| Surgeon 19 | 3 | 4 |
| Surgeon 20 | 2 | 2 |
| Layman 16 | 2 | 3 |
| Layman 17 | 2 | 4 |
| Layman 18 | 3 | 4 |
| Layman 19 | 4 | 4 |
| Layman 20 | 3 | 4 |

Evaluating the distribution of evaluations in the four results present in the form (1- Poor; 2- Fair; 3- Good; 4- Excellent), it is observed that 50% of the surgeons’ evaluators reported good and excellent results when they observed the photograph only of the post-operative period. -operative (Question 1), and only 35% of lay people reported this result. When both evaluators were exposed to the initial defect and could compare the results obtained (Question 2), there was an increase in the levels of evaluation of the operative result (Table 2).
| Evaluation | Layman | Surgeon | ||
|---|---|---|---|---|
| Question 1 | Question 2 | Question 1 | Question 2 | |
| 1- Bad | 10% (2) | 0% (0) | 5% (1) | 0% (0) |
| 2- Regular | 55% (11) | 30% (6) | 45% (9) | 20% (4) |
| 3- Good | 20% (4) | 30% (6) | 40% (8) | 35% (7) |
| 4- Excellent | 15% (3) | 40% (8) | 10% (2) | 45% (9) |

As for the assessments received by each ear individually, it was possible to notice that Ears 3 and 4 received higher median scores than Ears 1 and 2. This difference occurred in Question 1 and Question 2 (Table 1). Comparing the etiology of each defect with the results of the evaluations, defects resulting from auriculo-condylar syndrome had better results than defects resulting from trauma. This fact can be explained by the greater regularity of the defect in the auriculo-condylar syndrome, facilitating reconstruction and improving the operative and aesthetic results.
DISCUSSION
Techniques for reconstructing partial external auricular defects fall into two main categories. The first requires tissue removal, resulting in asymmetrical and smaller ears. And the second, with the interposition of grafts, flaps or both, is to maintain tissue volume.
Steffanoff described the retroauricular tubular flap in 1948, with a size of 16 x 68 mm. The anterior incision was made 8mm posterior to the cephaloauricular angle, and the posterior incision was made to provide 16mm of width to the graft. Support came from a cartilaginous graft from the concha of the ipsilateral ear, measuring 15mm wide by 56mm long. Eight surgical times were required to release the flap4.
In 1966, Cosman & Crikelair5 used a three-stage “composite tube” technique consisting of a superficial pedicle of the artery and temporal vein without an attached flap and covering it with a skin graft, with the disadvantages of leaving a hairless scar on the scalp and skin graft dyschromia.
Converse and Brent6 indicated a variety of techniques using tubular pedicles and suggested that the skin of the cephaloauricular sulcus could be the preferred location for flap design. Lewin7 used a similar strategy, only closing the flap donor site with a skin graft.
With the advancement of surgical knowledge, the techniques were adapted. Dujon and Bowditch reported that in 1995, three cases of helix defects caused by trauma were reconstructed using a modification of the Steffanoff technique in three surgical stages2. All the articles exposed cite good results and aesthetic improvement of the deformity after surgery using the tubular flap technique.
There is still the option of using cartilage grafts to reconstruct the defect in cases of greater loss of ear support, such as when the irregularity includes the anti-helix. When used, its insertion takes place in the first stage, during the tunnel’s construction and must remain for at least three weeks to ensure nutrition. The donor area is usually the contralateral ear. If the failure is small to intermediate, the formed tube maintains its shape without cartilage, aided by the fibrosis that forms in the post-operative period8.
In the present study, we evaluated the final operative result with two questions: Question 1, by showing only the post-operative photo, aimed to make the participant compare the aesthetic result with a normal ear; Question 2, on the other hand, revealed the
preoperative image and thus brought to the assessment an improvement concerning the original ear defect.
The option of initially exposing the post-operative photo without showing the initial defect was made to avoid creating a bias on the part of the evaluator in comparing the improvement obtained, giving a higher score in the post-operative period. Plastic surgeons and the lay population were included in the study as participants to seek assessments that reflected not only the views of specialists in the field but also of the general population.
In Question 1, the aesthetic result was rated as fair (grade 2) by 55% of lay participants and 45% of plastic surgeons and answered as good or excellent (grades 3 and 4) by 35% of laypersons and 50% of surgeons. In Question 2, there was an improvement in the evaluations, with no participant reporting it as bad (grade 1), 30% of lay people and 20% of surgeons judged it as fair (grade 2), and 70% of lay people and 80% of surgeons rated it as good or excellent (grades 3 and 4).
When comparing the evaluations obtained in questions 1 and 2, we noticed that when they knew about the previous defect, 55% of lay people and 65% of surgeons gave a higher grade to Question 2 than they had given to Question 1, evidencing that the knowledge of the previous defect influences the perception of the final result. Altogether, 75% of the participants considered the operative result (Question 2) good or excellent, and 56% characterized it as excellent, thus reinforcing the satisfactory post-operative aesthetic result already exposed by the patients.
Initially, the researchers expected that plastic surgeons would be more discerning than laypersons in their assessments, being better able to identify esthetic imperfections from their experiences. However, the opinions of laypeople were, on average worse than those of surgeons. A possible explanation is that when questioned in Question 1, surgeons perceived that it was a reconstructed ear, inferring a previous defect and generating a bias, while laypersons compared its aesthetics with that of a normal ear.
Our results allow us to indicate the tubular flap for patients with defects in the helix region and practically without reaching the anti-helix. Cases with greater involvement of the anti-helix should receive cartilage grafting to prevent the ear width from becoming too small and distorting the shape.
Recent reports on pedicled retroauricular flaps show that this option is simple, safe and aesthetically appropriate3,8,9, which corroborates the opinion of the participants, plastic surgeons, and laypeople questioned in this study.
CONCLUSION
We recommend this technique for reconstructing defects of variable helix edge sizes, regardless of etiology. It is a safe, reliable method with an adequate aesthetic result and minimal local morbidity.
REFERENCES
1. Siegert R, Magritz R. Otoplasty and Auricular Reconstruction. Facial Plast Surg. 2019;35(4):377-86. DOI: 10.1055/s-0039-1693745
2. Dujon DG, Bowditch M. The thin tube pedicle: a valuable technique in auricular reconstruction after trauma. Br J Plast Surg. 1995;48(1):35-8. DOI: 10.1016/0007-1226(95)90028-4
3. Masud D, Tzafetta K. The ‘double headed slug flap’: a simple technique to reconstruct large helical rim defects. Br J Plast Surg. 2012;65(10):1410-3. DOI: 10.1016/j.bjps.2012.03.048
4. Seffanoff DN. Auriculo-mastoid tube pedicle for otoplasty. Plast Reconstr Surg. 1948;3(3):352-60.
5. Cosman B, Crikelair G F. The composed tube pedicle in ear helix reconstruction. Plast Reconstr Surg. 1966;37(6):517-22.
6. Tanzer RC, Bellucci RJ, Converse JM, Brent B. Deformities of the auricle. In: Converse JM, ed. Reconstructive Plastic Surgery. Philadelphia: Saunders; 1977. p. 1671-3.
7. Lewin ML. Formation of the helix with a post-auricular flap. Plast Reconstr Surg. 1950;5:432-40.
8. Ellabban MG, Maamoun MI, Elsharkawi M. The bi-pedicle post-auricular tube flap for reconstruction of partial ear defects. Br J Plast Surg. 2003;56(6):593-8. DOI:10.1016/S0007-1226(03)00222-4
9. Cerci FB. Staged retroauricular flap for helical reconstruction after Mohs micrographic surgery. An Bras Dermatol. 2016;91(5 suppl 1):144-7. DOI:10.1590/abd1806-4841.20164733
1. Universidade Federal do Paraná, Curso de Medicina, Curitiba, PR, Brazil.
2. Universidade Federal do Paraná, Hospital de Clínicas, Universidade Federal do Paraná,
Curitiba, PR, Brazil.
3. Centro de Atendimento Integral ao Fissurado Lábio Palatal, Curitiba, PR, Brazil.
4. Hospital Erasto Gaertner, Curitiba, PR, Brazil.
RSF Conception and design study, Conceptualization, Final manuscript approval, Methodology, Project Administration, Supervision, Writing - Original Draft Preparation, Writing - Review & Editing.
CMG Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Methodology, Project Administration, Writing - Original Draft Preparation, Writing - Review & Editing.
SHM Analysis and/or data interpretation, Conception and design study, Conceptualization, Data Curation, Final manuscript approval, Methodology, Project Administration, Writing - Original Draft Preparation, Writing - Review & Editing.
Corresponding author: Caio Munaretto Giacomazzo R. General Carneiro, 181, Alto da Glória, Curitiba, PR, Brazil Zip Code: 80060-900 E-mail: caiomunagiaco@gmail.com
Article received: May 05, 2021.
Article accepted: December 13, 2021.
Conflicts of interest: none.
Institution: Universidade Federal do Paraná, Hospital de Clínicas, Departamento de Cirurgia Plástica, Curitiba, PR, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket