



Case Report - Year 2022 - Volume 37 -
Giant lipoma: surgical treatment
Lipoma gigante: tratamento cirúrgico

ABSTRACT
Introduction: Giant lipomas (>1000g), although rare, have relevant medical importance, as they can affect any region of the body and are diagnosed in advanced stages, in which there is functional impairment. They can also be confused with malignant soft tissue neoplasms. Furthermore, the natural history of the emergence and evolution of giant lipomas is still not exactly known, which justifies further studies. The current study aims to present the results of the surgical treatment of a case of giant lipoma.
Case Report: Case report that occurred in the plastic surgery service of the Roberto Santos Hospital in Salvador, Bahia, in the year 2016. A 62-year-old male farmer, 1.80 m tall, 74 kg, with a dorsal tumor measuring 35 cm in diameter, evaluated through clinical history and computed tomography examination and submitted to elliptical excision and plastic closure in W. There were no postoperative complications. Histopathology confirmed the diagnosis of giant lipoma (2881g). Post-surgical results were considered excellent by the patient and surgical team.
Conclusion: The giant lipoma was satisfactorily removed without complications, with excellent functional and aesthetic results.
Keywords: Case reports; Adipose tissue; Lipoma; Neoplasms, connective and soft tissue; Reconstructive surgical procedures
RESUMO
Introdução: Lipomas gigantes (>1000g), embora raros, têm importância médica relevante, pois podem acometer qualquer região do corpo e ser diagnosticados em fases avançadas, nas quais há comprometimento funcional. Eles também podem ser confundidos com neoplasias malignas de tecidos moles. Ademais, a história natural de surgimento e evolução de lipomas gigantes ainda não é exatamente conhecida, o que justifica a realização de estudos adicionais. O objetivo do corrente estudo é apresentar os resultados do tratamento cirúrgico de um caso de lipoma gigante.
Relato de Caso: Relato de caso ocorrido no serviço de cirurgia plástica do Hospital Roberto Santos em Salvador, Bahia, no ano de 2016. Homem de 62 anos, lavrador, 1,80m de altura, 74kg, com tumoração dorsal de 35cm de diâmetro, avaliado por meio de história clínica e exame de tomografia computadorizada e submetido a excisão elíptica e fechamento em plástica em W. Não houve complicações pós-operatórias. A histopatologia confirmou o diagnóstico de lipoma gigante (2881g). Os resultados pós-cirúrgicos foram considerados excelentes pelo paciente e equipe cirúrgica.
Conclusão: O lipoma gigante foi removido satisfatoriamente sem complicações, com excelentes resultados funcionais e estéticos.
Palavras-chave: Relatos de casos; Tecido adiposo; Lipoma; Neoplasias de tecido conjuntivo e de tecidos moles; Procedimentos cirúrgicos reconstrutivos
INTRODUCTION
Lipomas are benign neoplasms histologically characterized by the presence of mature adipocytes with small nuclei pushed to the cellular periphery by lipid droplets1,2. The tumor presents variable amounts of fibrous stroma, sometimes condensed in the lesion’s periphery, forming an incomplete capsule (pseudocapsule)3. Lipomas are the most frequent benign soft tissue mesenchymal tumors4,5,6, with an estimated incidence in the adult population of 0.21% to 0.5% and a prevalence of 10%7,8,9,10,11.
Lipomas are usually subcutaneous, but they can be located anywhere in the body that contains adipose tissue, including viscera, cavities, central nervous system, gastrointestinal tract, muscles and joints1,4,5,8.0 About 80% are smaller than 5 cm in diameter; however, some can reach more than 20 cm and weigh several kilograms, configuring the so-called giant lipomas5. Diagnosis of lipomas is clinical-histopathological1, and treatment is usually surgical7.
According to Sanchez et al.12, for a lipoma to be considered giant (GL), it must have a minimum of 10 cm in one of its dimensions or weigh at least 1000 grams. The largest reported GL in the world was 22.7kg5,12 and, in Brazil, 22.0kg8.
GL are uncommon in clinical practice (< 5% of all lipomas)4. Although rare, they have medical relevance, as they can affect any body region and are diagnosed in advanced stages in which there is aesthetic and/ or functional impairment4,5,6,9. They can be confused with malignant soft tissue neoplasms11,13. Finally, GL’s natural history is still not exactly known4.
OBJECTIVE
This work aims to report a case of GL treated with elliptical excision by the plastic surgery team at Hospital Roberto Santos (Salvador/BA) in 2016.
CASE REPORT
The report followed the recommendations of SCARE (Statement Consensus Based Surgical Case Report Guidelines 2018). The retrospective study was approved by the Medical Ethics Committee (CAAE 46603221.7.0000.5028, opinion 4.793.410).
Male, 62 years old, faioderm, farmer, 74kg, 1.80m, with a voluminous dorsal tumor that started 20 years earlier as a small bulge of slow and progressive growth, reaching its current dimensions five years ago. Since then, the patient has experienced local pain, grotesque deformity and social isolation.
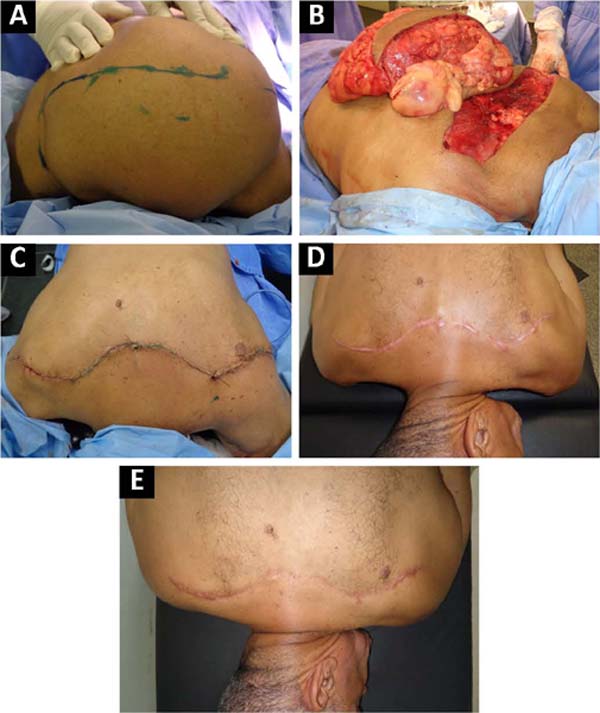
On examination, a hemispherical mobile mass measuring 35 cm in diameter was observed in the proximal third of the back, not adhering to deep planes, painless, softened, with normal overlying skin (Figure 1A). No abnormalities were found in family history, general physical examination or laboratory evaluation (blood count, coagulogram, blood glucose, urinalysis, urea, creatinine, electrolytes and ECG).
Multislice CT of the chest (Toshiba Aquilion 8-slice) revealed a multiseptated subcutaneous mass with fat density, measuring 21.0 x 23.1 cm, located in the upper third of the dorsum compatible with GL. The examination did not detect compression of thoracic or cervical structures.
The treatment instituted was surgical excision. Thirty minutes before the procedure, intravenous antibiotic prophylaxis (cefazolin, 2,000mg) was performed. However, drug thromboprophylaxis was not performed due to the low risk of developing intraoperative thrombosis (according to the criteria and recommendations proposed by Moulim et al.)14.
Under general anesthesia, a 30cm x 5cm transverse elliptical incision was made over the tumor dome, which was dissected from the surrounding subcutaneous and muscular tissues. The mass had a greasy appearance and consistency and had internal septa and a fibrous external capsule forming a cleavage plane (except on the deep side of the tumor) that facilitated dissection and resulted in limited bleeding. A massive multilobed lipomatous tumor was removed (Figure 1B), showing its paravertebral emergence from the middle part of the left trapezius (Figure 1B - arrow). After hemostasis, excess skin was removed and closed with an inverted W suture (Figure 1C). Stitches were made with 2-0 black mononylon thread in subdermal (simple inverted) and intradermal (continuous cuticular suture) planes.

The entire procedure, including skin suturing, lasted four hours and thirty minutes and was performed by a team coordinated by a plastic surgeon with 20 years of training in the specialty. The patient was discharged from the hospital after seven days of uncomplicated hospitalization. Postoperatively, he was instructed to apply wet gauze dressings and antibiotic ointment (bacitracin and neomycin) until complete healing, followed up on an outpatient basis by the surgical team weekly for the first month and then every two months.
Histopathological analysis revealed a giant lipoma measuring 2881 grams, measuring 29.0 x 26.0 x 6.0 cm. In the sixth month evaluation, the operated region remained flat, with a slightly hypertrophic surgical scar (5mm, Figure 1D) and slightly depressed in the 5-year evaluation (Figure 1E). The patient and the surgical team considered the final result (aesthetic and functional) excellent.
DISCUSSION
The current report presents a typical patient with GL: a male in the sixth decade of life with a slow-growing tumor and unrecognizable etiology1,4,5,6,9,11,13. The lipoma’s dimensions and mass (2881g), although reduced concerning the bulkier GLs described, fit into the most common range described for GL (493.75g to 3.8 kg-cm)11. The preoperative diagnosis of the present GL was clinical, as the lesion had the usual characteristics (soft consistency, slow growth, mobility and intact overlying skin, absence of pain and systemic manifestations15).
The GL presented was an example of an inter-muscular lipoma related to the trapezius. Interestingly, the first subfascial lipoma described in the literature (in 1856, by Padget) also originated from the muscle3. When growing, the GL of the current report caused great expansion of the overlying skin, so there was a need to remove a large ellipse of redundant integument after removing the mass. The final suture was placed in a zigzag pattern to prevent retractable straight scar formation. The long surgical time was attributed to the large size of the tumor and the difficulty in releasing the GL attached bilaterally to the underlying trapezius due to the absence of an identifiable fibrous capsule in the area of contact with the muscle.
The GL described did not present compressive symptoms, so the excision was performed to allow a differential diagnosis with liposarcomas and, above all, for cosmetic reasons. Rydholm & Berg reported that lesions >10 cm have a 25-fold greater risk of malignancy than lesions <5 cm. This study alerts to the need for surgical removal of the GL even in the absence of manifestations suggestive of malignancy7. Despite the compressive problems they may cause, paradoxically, most lipomas are removed for aesthetic reasons4. As in a current report, the indication can be important for correcting gross deformities, contributing to the reintegration of patients socially marginalized because of the deformity.
The present report’s lack of postoperative adverse effects seems to be an exceptional finding, since immediate complications after GL resection are frequent, including paresthesias, skin necrosis, surgical wound infections, lower limb varicose veins and pulmonary complications8. Late postoperative complications have not been reported5. Post-surgical relapses are considered low for the intermuscular variant and slightly higher for the intramuscular type, especially when the affected muscles are preserved4,11,13.
CONCLUSION
The presented GL was removed without complications and with excellent aesthetic and functional results.
REFERENCES
1. Nigri G, Dente M, Valabrega S, Beccaria G, Aurello P, D’Angelo F, et al. Giant inframuscular lipoma disclosed 14 years after a blunt trauma: a case report. J Med Case Rep. 2008;2:318.
2. Righi A, Pantalone O, Tagliaferri G. Giant lipoma of the thigh: a case report. J Ultrasound. 2012;15(2):124-6.
3. Kindblom LG, Angervall L, Stener B, Wickbom I. Intermuscular and intramuscular lipomas and hibernomas. A clinical, roentgenologic, histologic, and prognostic study of 46 cases. Cancer. 1974;33(3):754-62.
4. Daher JC, Amaral JDLG, Cammarota MC, Benedik Neto A, de Faria CADC. Lipoma gigante de Membro inferior com repercussão no sistema vascular. Rev Bras Cir Plást. 2013;28(3):522-5.
5. Accetta P, Accetta I, Vassallo EC, Milman M, Souza AM, Accetta AC. Lipomas gigantes. Rev Col Bras Cir. 1998;25(5):364-5.
6. Hakim E, Kolander Y, Meller Y, Moses M, Sagi A. Gigantic lipomas. Plast Reconstr Surg. 1994;94(2):369-71.
7. Rydholm A, Berg NO. Size, site and clinical incidence of lipoma. Factors in the differential diagnosis of lipoma and sarcoma. Acta Orthop Scand. 1983;54(6):929-34.
8. Mello D F, Manica MZ, Helene Júnior A. Lipomas gigantes: série de 14 casos. Rev Bras Cir Plást. 2015;30(1):33-7.
9. Mello D, Helene A Jr. Lipoma subgaleal gigante: relato de caso. Rev Bras Cir Craniomaxilofac. 2010;13(3):180-2.
10. Mescon H. Lipoma in clinical dermatology. Clin Dermatol. 1991;4:1-2.
11. Terzioglu A, Tuncali D, Yuksel A, Bingul F, Aslan G. Giant Lipomas: A series of 12 consecutive cases and a giant liposarcoma of the thigh. Dermatol Surg. 2004;30(3):463-7.
12. Sanchez MR, Golomb FM, Moy JA, Potozkin JR. Giant lipoma: case report and review of the literature. J Am Acad Dermatol. 1993;28(2 Pt 1):266-8.
13. d’Alessandro G, Nunes T, Lajner A, Beirigo M, Porto O, Pinto W. Lipoma intermuscular gigante: relato de caso. Rev Bras Cir Plást. 2008;23(3):226-8.
14. Moulim JL, Sobreira ML, Malgor RD, de Abreu CR, de Araújo ESF, Palhares Neto AA. Estudo comparativo entre protocolos para profilaxia da trombose venosa profunda: uma nova proposta. Rev Bras Cir Plást. 2010;25(3):415-22.
15. Singh M, Saxena A, Kumar L, Karande SK, Kolhe Y. Giant Lipoma of Posterior Cervical Region. Case Rep Surg. 2014;2014:289383.
1. Instituto de Ciências da Saúde, Universidade Federal da Bahia, Programa de Pós-Graduação
em Processos Interativos de Órgãos e Sistemas, Salvador, BA, Brazil.
2. Hospital Geral Roberto Santos, Cirurgia Geral, Salvador, BA, Brazil.
SCS Analysis and/or data interpretation, Conception and design study, Conceptualization, Final manuscript approval, Formal Analysis, Investigation, Methodology, Project Administration, Supervision, Writing - Original Draft Preparation, Writing - Review & Editing.
RAV Final manuscript approval, Realization of operations and/or trials.
Corresponding author: Sandro Cilindro de Souza ICS-UFBA, Av. Reitor Miguel Calmon, sala 110, 1º Andar, Vale do Canela, Salvador, BA, Brazil Zip Code: 40110-902 E-mail: sandrocilin@gmail.com.br
Article received: April 26, 2021.
Article accepted: October 15, 2021.
Conflicts of interest: none.
Institution: Hospital Geral Roberto Santos, Salvador, BA, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket