



Ideas and Innovation - Year 2022 - Volume 37 -
Concomitant use of elastic suture associated with vacuum dressing in the closure of large soft tissue losses
Uso concomitante de sutura elástica associada ao curativo a vácuo no fechamento de grandes perdas de partes moles
Antoninho José Tonatto Filho1,2* ; Jorge Luis de Moraes1,2; Caio Munaretto Giacomazzo3; Alessandra Bossardi4; Marlon Câmara Lopes1,2; Renato da Silva Freitas1,2
; Jorge Luis de Moraes1,2; Caio Munaretto Giacomazzo3; Alessandra Bossardi4; Marlon Câmara Lopes1,2; Renato da Silva Freitas1,2
ABSTRACT
Treating complex wounds with great loss of soft tissues is a challenge for plastic surgery, especially when the wound is infected. Several options are considered for treatment, such as sutures, grafts, flaps, and expanders. Due to the complexity of the cases, the frequent association of morbidities, the need for multidisciplinary interventions, and long hospital stays, treatment costs are often high. This work demonstrates the elastic suture technique used in a clinical case, using continuous skin traction in association with a vacuum dressing, which enabled patient rehabilitation without the need for more aggressive interventions to close the extensive traumatic wound.
Keywords: Sutures; Vacuum; Wound closure techniques; Suture techniques; Soft tissue injuries.
RESUMO
O tratamento das feridas complexas com grande perda de partes moles é um desafio para a cirurgia plástica, principalmente quando a ferida encontra-se infectada. Várias opções são consideradas para o tratamento, como sutura, enxertos, retalhos, expansores. Devido à complexidade dos casos, frequente associação de morbidades, necessidade de intervenções multidisciplinar e longos internamentos, os custos do tratamento são frequentemente elevados. Este trabalho vem demonstrar a técnica de sutura elástica empregada em um caso clínico, utilizando tração contínua da pele em associação ao curativo a vácuo, que possibilitou reabilitação do paciente sem a necessidade de intervenções mais agressivas para o fechamento da ferida traumática extensa.
Palavras-chave: Suturas; Vácuo; Técnicas de fechamento de ferimentos; Técnicas de sutura; Lesões dos tecidos moles.
INTRODUCTION
Treating complex wounds with great soft tissue loss is a challenge for plastic surgery, especially when the wound is infected. In the literature, we find numerous already established techniques, with their benefits and disadvantages, such as grafting, flaps, tissue expanders and elastic suture.
The decision for the technique to be used is essential for successful reconstruction, and, based on the principle that the best repair is always the simplest1, the fundamentals of reconstructive surgery were created. Therefore, primary wound closure is the first choice whenever possible.
Raskin used an elastic suture for the first time in 1993 to approximate the borders of a post-compartment syndrome fasciotomy in an upper limb2. The principle was based on the fixation with the tension of an interlaced elastic, fixed to the edges of the skin, making a continuous tension of the skin, putting into practice the concept of elasticity and skin compliance. It can be used to close different skin defects resulting from different causes, such as car accidents, resections of skin lesions and tissue necrosis. Elastic suture, as an alternative for treating the acute phase of skin loss, is a simple, low-cost procedure that provides good results for cases of tissue loss3.
In 1996, Leite revised the technique after observing the incidence of skin necrosis at the edges of the wound, using the Raskin technique, and then proposed fixing the elastic in the subcutaneous and superficial fascia, sparingly the skin from the ischemic event induced by tensile force4.
The use of vacuum dressing, whose description in animal studies dates back to the 1970s5, has established itself as an important alternative in treating complex wounds, including for the pediatric population6. It is a system used in wound healing in which localized and controlled negative pressure is instituted to stimulate granulation and healing. Negative pressure promotes arterial vasodilation and, consequently, increases blood flow in the tissues, stimulating the formation of granulation scar tissue. Fluid removal decreases edema, interstitial pressure, and bacterial colonization, creating a moist environment beneficial for epithelial migration and healing. In addition, it produces traction on the wound’s edges, reducing its dimension7.
Thus, this work aimed to combine the benefits of elastic suture and vacuum dressing with a more comprehensive approach to a complex infected wound with great loss of soft parts of the lower limb.
METHODS
This is a retrospective, observational study of a patient who underwent reconstruction of the right lower limb using an elastic suture and a vacuum dressing at Hospital do Trabalhador, in Curitiba-PR, in 2020. Study approved by the Ethics Committee on Search under CAAE 52792121.7.0000.5225.
Patient DGLD, male, 20 years old, previously healthy, is referred to the Emergency Department of the Hospital do Trabalhador in Curitiba, victim of a collision between a motorcycle and a car. He is admitted to the emergency room with a significant laceration on the right lower limb, extending from the knee to the distal third of the leg, with no signs of fracture on radiography.
Upon admission, the patient underwent debridement and containment of the edges with sterile plastic (Figure 1) by the orthopedics team, who requested a follow-up by the Plastic and Reconstructive Surgery Service. On the seventh day of hospitalization, the patient underwent a new surgical procedure by the plastic surgery team. A large clot was identified, exhaustive washing was performed, and hemostasis was reviewed (Figure 2).




In the transoperative period, it was decided to perform the elastic suture associated with the vacuum dressing (Figure 3), with a surgical reassessment plan and new reconstruction plan after 7 days, when the rotation of the myocutaneous flap for closure was considered. In the surgical reassessment, with satisfactory evolution of the wound, it was decided to maintain the conduct of the elastic suture and vacuum therapy treatments.


The patient underwent two more approaches with an interval of 7 days, with this association, with gradual wound closure (Figure 4) until the edges’ final primary suture and elastics’ removal (Figure 5). Patient, coming from another state, chose to end treatment in his hometown, without new procedures. Photo, after contact with it, is in Figure 5.




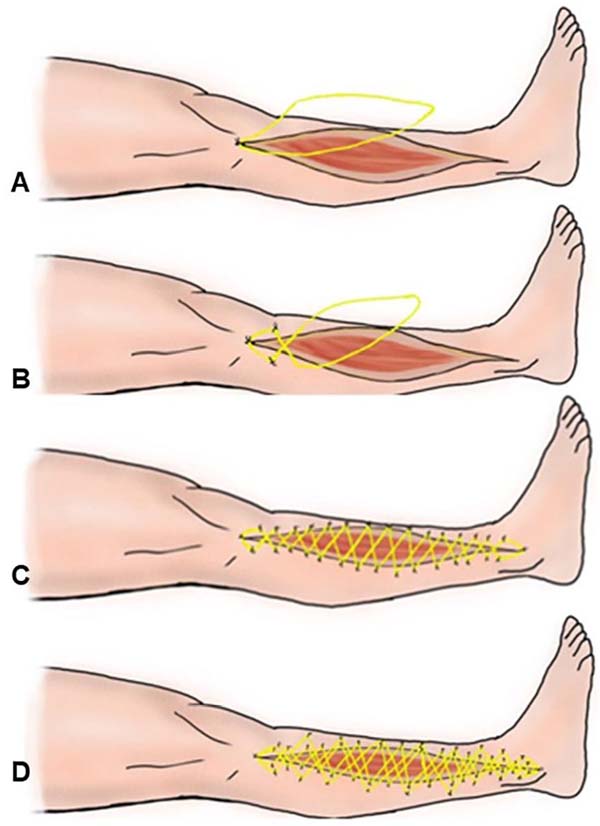
The demonstration of how the elastic suture is performed can be seen in Figure 6.

DISCUSSION
Complex wounds are the most challenging and often require a surgical approach. Wound care aims to create a favorable environment for wound healing or coverage, and debridement is the basis for most strategies. Primary synthesis, secondary synthesis, grafts, local flaps, regional flaps, and free flaps are included from the simplest to the most complex steps. When choosing the procedure, one should consider the best option to maintain the shape and function of the region to be reconstructed8.
In the case in question, the elastic suture in association with the vacuum dressing was effective in helping to definitively close the lesion, dispensing with the use of skin autograft, flaps, or tissue expansion9. The open wound is maintained under elastic tension, which was exerted by sterile rubber bands, performed by suturing the rubber with 2.0 and 3.0 nylon stitches attached to the viable skin tissue. It starts with a stitch at the end of the wound and then one on each side on the opposite skin edges after braiding the elastic at 180º, successively repeating until the end of the incision.
During the treatment sequence, elastics sutured with Nylon 2-0 further away from the edges were used to reduce the tension of the edges of the wound, thus avoiding cutaneous vascular suffering, which was jointly benefited by the arterial vasodilation resulting from the dressing to concomitant vacuum. During each procedure, sterile rubbers were replaced with new ones to maintain effective tension and a new vacuum dressing.
After improving the tension of the wound by continuous traction and negative pressure, it was possible to perform the primary suture of the lesion.
CONCLUSION
The use of continuous traction elastic suture associated with a vacuum dressing made it possible to close a complex wound on the lower limb without the need for rotation of the myocutaneous flap and other sequelae, proving to be an alternative with lower morbidity for the case demonstrated.
REFERENCES
1. Mathes SJ, Nahai F. Reconstructive Surgery: Principles, Anatomy Techinique. New York: Churchill Livingstone and Qualit Medical Publishing; 1997.
2. Raskin KB. Acute vascular injuries of the upper extremity. Hand Clin. 1993;9(1):115-30.
3. Vidal MA, Mendes Junior CES, Sanches JA. Sutura elástica - uma alternativa para grandes perdas cutâneas. Rev Bras Cir Plást. 2014;29(1):146-50.
4. Leite NM, Reis FB, Christian RW. Tratamento de ferimentos deixados abertos com o método da sutura elástica. Rev Bras Ortoped. 1996;31:687-9.
5. Morykwas MJ, Argenta LC, Shelton-Brown EI, McGuirt W. Vacuum-assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg. 1997;38(6):553-62.
6. Baharestani MM. Use of negative pressure wound therapy in the treatment of neonatal and pediatric wounds: a retrospective examination of clinical outcomes. Ostomy Wound Manage. 2007;53(6):75-85.
7. Oliveira MSL, Komatsu CA, Ching AW, Faiwichow L. Tratamento de feridas complexas com uso de pressão negativa local método a vácuo. Rev Bras Cir Plást. 2010;25(3 Suppl 1):66.
8. Petroianu A, Sabino KR, Alberti LR. Closure of large wound with rubber elastic circular strips - case report. Arq Bras Cir Dig. 2014;27(1):86-7. DOI: 10.1590/s0102-67202014000100021
9. Teixeira Neto N, Chi A, Paggiaro AO, Ferreira MC. Surgical treatment of complex wounds. Rev Med (São Paulo). 2010;89(4/4):147-52.
1. Hospital de Clínicas de Curitiba, Curitiba, PR, Brazil
2. Hospital do Trabalhador, Curitiba, PR, Brazil
3. Universidade Federal do Paraná, Curitiba, PR, Brazil
4. Universidade de Caxias do Sul, Caxias do Sul, RS, Brazil
AJTF Conception and design study, Conceptualization, Formal Analysis, Methodology, Writing - Original Draft Preparation, Writing - Review & Editing.
JLM Conception and design study, Methodology, Writing - Original Draft Preparation.
CMG Final manuscript approval, Project Administra- tion, Writing - Original Draft Preparation.
AB Writing - Original Draft Preparation, Writing - Review & Editing.
MCL Conception and design study, Conceptualization, Formal Analysis, Supervision, Writing - Review & Editing.
RSF Conception and design study, Formal Analy- sis, Supervision, Writing - Review & Editing.
Corresponding author: Antoninho José Tonatto Filho Rua General Carneiro, 181, Setor/sala de Cirurgia Plástica, 9º andar, Alto da Glória, Curitiba, PR, Brazil. Zip Code: 80060-900, E-mail: aj.tonatto@gmail.com
Article received: October 18, 2020.
Article accepted: September 13, 2022.
Conflicts of interest: none.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket