



Case Report - Year 2023 - Volume 38 -
Method of closing fasciotomies by progressive tissue traction
Método de fechamento de fasciotomias por tração tecidual progressiva
Antoninho José Tonatto1,* ; Jorge Luís de Moraes1; Caio Munaretto Giacomazzo3; Bruna Valduga Dutra4; José Paulo Tapie Barbosa2; Renato da Silva Freitas1
; Jorge Luís de Moraes1; Caio Munaretto Giacomazzo3; Bruna Valduga Dutra4; José Paulo Tapie Barbosa2; Renato da Silva Freitas1
ABSTRACT
High-energy trauma has increased significantly in the last decade, mostly in the lower limbs, in many cases requiring fasciotomy due to the subsequent compartment syndrome. In this context, its closure often leads to a delay in the patient's comprehensive treatment and the return to their activities and may lead to local infection, in addition to generating high costs. There are many options for the plastic surgeon to try to bring the edges together and reconstruct the extremities, such as flaps, grafts, vacuum dressings, and elastic sutures, in addition to expansion devices, sometimes with a combination of the above.
Keywords: Sutures; Fasciotomy; Traction; Kirschner wire; Wound closure techniques
RESUMO
O trauma de grande energia vem aumentando de maneira expressiva na última década, em boa parte de membros inferiores, necessitando, em muitos casos, de fasciotomia devido à síndrome compartimental subsequente. Neste contexto muitas vezes seu fechamento acaba por levar a um retardo no tratamento integral do paciente, do retorno a suas atividades e podendo levar a infecção local, além de gerar altos custos. Há muitas opções ao cirurgião plástico para a tentativa de aproximação de bordos e reconstrução das extremidades, como retalhos, enxertos, curativo a vácuo e sutura elástica, além de dispositivos de expansão, sendo, às vezes, com combinação das anteriores. O método de fechamento apresentado através do alongamento progressivo da pele com fio de Kirschnner representa uma forma de baixo custo e facilmente reproduzível para lidar com este tipo de ferida.
Palavras-chave: Suturas; Fasciotomia; Tração; Fio de Kirschner; Técnicas de fechamento de ferimentos
INTRODUCTION
High-energy trauma has increased significantly in recent decades, mainly due to motorcycle and car accidents. Trauma victims may present varying severity and location injuries, with the lower limbs being an important and common site affected. These can range from simple skin continuity solutions to major tissue loss and exposure of noble structures1,2.
The decision for the technique to be used is essential for successful reconstruction, and, based on the principle that the best repair is always the simplest3, the fundamentals of reconstructive surgery were created. Therefore, primary wound closure is the first choice whenever possible.
However, in wounds with great loss of soft tissues, or when decompressive fasciotomy of the limbs is performed with local skin retraction and muscle protrusion, there is difficulty in performing such closure. Several alternatives are proposed for the closure of the extremity wound, such as grafts, flaps, elastic sutures, adhesive tapes, and plastic clamps, the former being able to be associated with the vacuum dressing.
Within this context, closure through intermittent traction with Kirschner wires and steel wires becomes a viable, inexpensive, low-morbidity option, avoiding new scars created by flap rotation that can result in retraction, ischemia, and tissue necrosis4,5, and being easy to reproduce for closing numerous limb wounds, as well as fasciotomies.
OBJECTIVE
The present study evaluates the closure of a post-trauma lower limb wound with local fasciotomy, through continuous and intermittent traction with a Kirschner wire associated with steel wires, as an alternative for highly complex injuries.
CASE REPORT
This is a retrospective, observational study of a patient who underwent fasciotomy closure through dermatotraction with steel wire at the Hospital do Trabalhador, in Curitiba-PR, in 2020. Study approved by the Research Ethics Committee, under CAAE 52788221.0.0000.5225.
Patient LFMP, male, 26 years old, previously healthy, comes to the emergency room at the Hospital do Trabalhador in Curitiba with a history of a fall from the same level into a maintenance hole, with consequent dislocation of the left knee joint. He preserved the posterior tibial artery, popliteal artery pulses, and anterior tibial artery pulse on admission. He was referred to the surgical center for dislocation reduction by the Orthopedics team. In the immediate postoperative period of transarticular external fixation, there was a slowdown in capillary refill time, the temperature difference concerning the contralateral limb, and difficulty in palpating pulses.
An assessment by the Vascular Surgery team was then requested, which on physical examination of the patient, found the absence of anterior tibial, posterior tibial, and popliteal pulse, pain on palpation of the calf, and decreased movement of the toes. Angiotomography was performed, which confirmed a lesion in the popliteal artery, and the patient was taken back to the surgical center for revascularization of the limb, with interposition of the popliteal artery with the reverse saphenous vein and medial and lateral fasciotomy.
During the postoperative period, the patient evolved with signs of reperfusion syndrome and was referred to the Intensive Care Unit (ICU). After 4 days, he was discharged from the ICU, maintaining decreased foot sensitivity and absent motricity in the toes and forefoot. Anterior and posterior tibial pulses are present, without popliteal pulse attributed to edema. Fluxes present on Doppler.
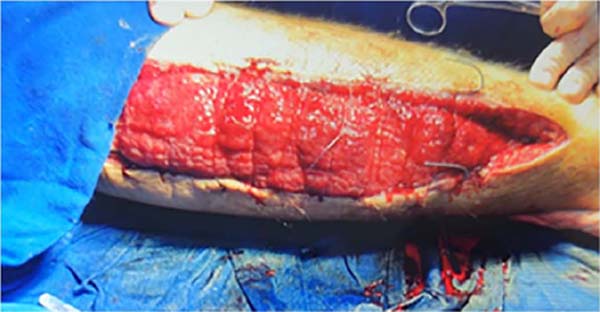
On the tenth postoperative day, the patient started with a fever, progressing to blisters and hallux necrosis. Ultrasonography was performed, which identified the presence of a collection in the distal third of the wound, which was drained with a large number of clots and a purulent collection. Subsequently, he was submitted to successive debridements of devitalized tissues due to muscle necrosis in the deep posterior compartment, interosseous membrane, and anterior compartment (Figure 1).


An evaluation was requested after the patient’s first vacuum dressing to monitor the condition, assessing the lesion (Figure 2) and indicating the approximation of the edges with 1.5 Kirschner wires in association with the twisting of 0 steel wires (Figure 3) in association with the dressing vacuum for drainage of secretion and approximation of borders. Four sessions were performed to approximate the edges by twisting the steel wires (Figure 4), all in a surgical center under spinal anesthesia; the mean interval between procedures was 3 days. Ultimately, the surgical wound was completely resolved with the proposed treatment (Figure 5), without grafts, flaps, or other procedures, ending the procedure with a primary suture of the lesion.







The time between the first intervention by the Plastic Surgery team and hospital discharge was two weeks. Thus, the various surgical times for tissue traction and approximation of the edges did not generate an extension of hospital stay.
The patient was followed up at the outpatient clinic for 12 months without suture dehiscence, local aesthetic complaints, or other complications inherent to the proposed treatment. He was satisfied with the final aesthetic result and was discharged from the service.
DISCUSSION
Due to the significant increase in high-energy trauma in recent decades, mainly due to motorcycle and car accidents, the number of complex fractures of extremities that are difficult to close is increasing. Many of them require fasciotomy, which momentarily becomes necessary, but can lead to difficulty in their primary suture, requiring flaps, grafts, vacuum dressing, elastic sutures, or other means for closing the same.
The number of fasciotomies registered in the Public Health System (SUS) in the last decade, 2009-2019, was 26,905 nationally, with 13,758 in the lower limbs6. Amid this, the plastic surgeon must have a range of alternatives to close fasciotomies. Among them, we found intermittent traction with Kirschner and steel wires a cheap method, easily reproducible by other surgeons, and of great value for this purpose. This technique is a variation based on tissue expansion described by Neuman in 1956, in which skin gain is obtained through slow and intermittent expansion7, by Bashir (1987)8 and Callanan & Macey (1997)9.
This expansion process can be explained by the phenomenon of mechanical drag, in which the collagen fibers stretch parallel to the direction of the traction force, and the fundamental substance, composed of mucopolysaccharides and tissue fluids, which, being displaced, leads to a final result of increased of surface area10,11,12,13.
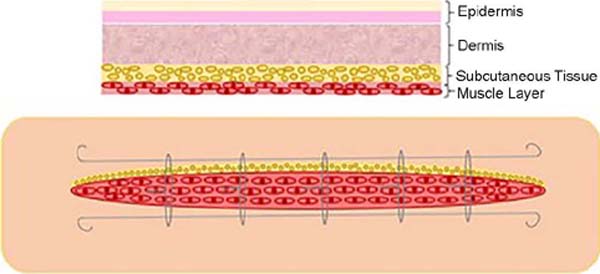
1-1.5mm Kirschner wires are passed through the healthy skin, being crossed parallel to the edges of the wound in the dermal plane, approximately 5-7mm from the edge of the wound, the remaining ends being cut and inverted, in order to support them and not lose them between its ends. Then, grade 0 steel wires are introduced through both Kirschner wires between the edges, and they are twisted and stretched to perform traction to approximate the edges. The steel wires are inserted longitudinally and parallel to the longest axis of the wound in the intradermal plane with a manually curved 18G needle. The representative scheme of how the method is performed can be seen in Figure 6.

Subsequently, every 2 - 3 days, as well as weekly, depending on the patient’s clinical status and tolerability, the steel wires are pulled again until the edges are ready for primary closure; the procedure can be performed in the operating room under anesthesia or intravenous sedation, or at the bedside with a locoregional blockade, depending on the patient’s pain tolerance.
During the traction of the evaluated case, ischemic suffering of the skin or other intercurrences were not evaluated, respecting the traction allowed according to the elasticity of the skin presented at each procedure.
A meta-analysis conducted by Jauregui et al.14 compared the various types of fasciotomy closure described in the literature, including conservative treatment (dressings only), partial skin grafts, elastic suture, gradual approximation, dynamic dermatotraction (with specific devices) and negative pressure, with the success rate defined as wound closure without the need for partial skin grafting. Dynamic dermatotraction with specific devices (92.7%) and gradual approximation techniques (92.4%) had the highest success rates. On the other hand, negative pressure dressings obtained the worst results, with 78.1% of success14.
Elastic suture, another inexpensive and easily reproducible modality, can gradually close complex wounds or fasciotomies. Raskin used it for the first time in 1993 to approximate the borders of a post-compartment syndrome fasciotomy in an upper limb15.
The principle was based on the fixation with the tension of an interlaced elastic, fixed to the edges of the skin, making a continuous tension of the skin, putting into practice the concept of elasticity and skin compliance. The technique was revised by Leite, in 1996, after observing the incidence of skin necrosis at the edges of the wound when using the Raskin technique; he then proposed the fixation of the elastic in the subcutaneous tissue and the superficial fascia, sparing the skin from the ischemic event induced by the tensile force15.
Meanwhile, traction with steel wires can be controlled, performing traction as needed so that vascularization, which is the limiting factor for skin traction in the various methods, can be performed without compromising. Thickness, skin tension of the displaced flap, skin pallor, and pain are the indicators to assess the ugly traction with the steel wires.
Another point that should be considered is the procedure’s low cost. While steel wires cost approximately R$5.00, other similar dermatotraction devices cost around US$500-1000, and negative pressure dressings around US$96 a day10. Other techniques to achieve skin gain through intraoperative distension, described by Hirshowitz et al.16, Stough et al.17, Lam et al.18, Bjarnesen et al.19 and others, require specialized equipment for their execution, being the former unavailable in most hospitals and being more expensive7.
Unlike tissue grafting, dermatotraction requires a longer hospital stay, especially in large wounds. In this case, dermatotraction was performed in a surgical center under anesthetic blockade via spinal anesthesia in all procedures; however, depending on the patient’s pain tolerance, it could be performed at the bedside.
We believe this method is valid mainly for patients needing to remain hospitalized for reasons other than closing the fasciotomy, especially if we consider that vacuum therapy cannot be performed at home in our country due to its unavailability in the Public Health System (SUS). In cases where the early discharge of the patient is possible, other methods, such as tissue grafting, should be considered.
CONCLUSION
The work demonstrates yet another highly valuable, safe, inexpensive, easily reproducible, and low-morbid alternative to the arsenal of techniques available to surgeons for closing fasciotomy and complex extremity injuries, often requiring prolonged hospitalization and difficult therapeutic management.
1. Hospital de Clínicas de Curitiba, Cirurgia Plástica, Curitiba, Paraná, Brazil
2. Hospital do Trabalhador, Cirurgia Plástica, Curitiba, Paraná, Brazil
3. Universidade Federal do Paraná, Curso de Medicina, Curitiba, Paraná, Brazil
4. Universidade de Caxias do Sul, Curso de Medicina, Caxias do Sul, Rio Grande do
Sul, Brazil
Corresponding author: Antoninho José Tonatto Filho Rua Ubaldino do Amaral, 124/701, Bairro Alto da Gloria, Curitiba, PR, Brazil. Zip code: 80060-190 E-mail: aj.tonatto@gmail.com
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket