



Original Article - Year 2023 - Volume 38 -
Postoperative radiotherapy with an electron beam on keloid scar: epidemiological evaluation in a teaching hospital
Radioterapia pós-operatória com feixe de elétrons sobre cicatriz queloideana: avaliação epidemiológica em hospital de ensino
Balduino Ferreira de Menezes1,* ; Lucas Vannuchi Magnani1; Batista de Oliveira2; Aristides Augusto Palhares1
; Lucas Vannuchi Magnani1; Batista de Oliveira2; Aristides Augusto Palhares1
ABSTRACT
Introduction: Keloids are one of the most aggressive spectrums of healing disorders. They have a unique pathophysiology and multiple specific genetic and cellular factors, which have not yet been fully elucidated. So far, literature reviews have found the influence of genetics, injury site, and ethnicity on the incidence and rate of recurrence. Furthermore, the need to associate an adjuvant method with surgical excision has already been verified, but the best therapy has yet to be defined.
Method: A retrospective analysis of medical records was carried out to assess the profile of patients who underwent postoperative radiotherapy with an electron beam to treat keloids at the Hospital das Clínicas da Faculdade de Medicina de Botucatu between 2015 and 2019.
Results: Data from 131 patients were evaluated, with 269 keloid scars treated. The average duration of treatment was 51 days, and the number of sessions was 17. White patients were predominant (78%) and women (70%), with surgical incision being the main cause of formation (49%) and ear the most identified location (33%). Women were more likely to complete the proposed treatment (p=0.04), while non-literates completed less than those who had at least completed primary or secondary education (p<0.0001).
Conclusion: Postoperative radiotherapy for keloid scars is a well-established treatment in the literature and an important tool for plastic surgeons. Knowing the profile of patients who need this therapy is essential to create methods that improve adherence and results.
Keywords: Keloid; Scar; Radiotherapy, adjuvant; Reconstructive surgical procedures; Medical records
RESUMO
Introdução: Os queloides correspondem a um dos espectros mais agressivos dos distúrbios da cicatrização. Possuem fisiopatologia ímpar e múltiplos fatores genéticos e celulares específicos, ainda não totalmente elucidados. Até o momento, revisões literárias encontraram influência da genética, local da lesão e etnia sobre a incidência e taxa de recorrência. Ademais, já foi constatada a necessidade de associação de um método adjuvante com a excisão cirúrgica, mas ainda sem definição da melhor terapia.
Método: Realizada uma análise retrospectiva de prontuários para avaliação do perfil dos pacientes submetidos a radioterapia pós-operatória com feixe de elétrons para o tratamento de queloides no Hospital das Clínicas da Faculdade de Medicina de Botucatu, entre 2015 e 2019.
Resultados: Foram avaliados os dados de 131 pacientes, com um total de 269 cicatrizes queloideanas tratadas. A média da duração do tratamento foi de 51 dias e do número de sessões, de 17. Houve predominância de pacientes brancos (78%) e de mulheres (70%), sendo incisão cirúrgica a principal causa de formação (49%) e a orelha a localização mais identificada (33%). As mulheres tiveram mais chance de completar o tratamento proposto (p=0,04), enquanto os não alfabetizados completaram menos do que aqueles que tinham pelo menos ensino fundamental ou médio completo (p<0,0001).
Conclusão: A radioterapia pós-operatória em cicatrizes queloideanas é um tratamento consagrado na literatura e uma importante ferramenta do cirurgião plástico. Conhecer o perfil dos pacientes que necessitam desta terapia é fundamental para criar métodos que melhorem a adesão e o resultado da mesma.
Palavras-chave: Queloide; Cicatriz; Radioterapia adjuvante; Procedimentos cirúrgicos reconstrutivos; Registros médicos
INTRODUCTION
Healing, a dynamic and multifactorial process divided into three phases – inflammatory, proliferative, and remodeling – is one of the most important defense mechanisms of the human body by preventing blood loss and ensuring tissue repair. However, as it is a dynamic process, several known and unknown factors can positively affect it, resulting in an adequate recovery of the injured tissue.
Thus, when the site is the skin, the aim is to return to the state as close as possible to the previous one, which, depending on the mechanism and type of trauma, is not achieved1. Despite all the efforts of the cellular recovery mechanism, many cases do not reach the desired aesthetic or functional appearance2.
From the classification of scars, it was possible to elaborate protocols for their treatment, which differ in light or more invasive therapies, depending on the severity of the case. Thus, because they are considered more severe, scars classified as keloids require different therapeutic strategies3, 4.
Keloids, first described and named by Alibert in 18065, were presented as a growth similar to the projection of branches or the claws of a crab, which from the Greek khele derived the English word keloid, being translated into Portuguese as queloide.
Considered a benign tumor, it is characterized by the expansion of the limits of the initial lesion with a prolonged course of activity, in addition to having a unique pathophysiology and multiple specific genetic and cellular factors, with many of its variables not yet fully understood6. At the histological level, there is a chronic inflammation of the reticular dermis, with increased fibroblasts and collagen, specifically type I, eosinophilic and hyalinized.
So far, it is known that there is a greater development and growth of keloids during puberty, in addition to an increase during pregnancy and a decrease after menopause7. Among the factors that promote its emergence, we can highlight genetics, the site of the initial lesion, and ethnicity8.
Although not yet fully elucidated, several findings suggest genetic influence as a predisposing factor to the formation of keloids. For example, some families have multiple members affected, and the prevalence in twins is more frequent. When evaluating such families, possible patterns of autosomal dominant heterogeneity are observed, but cases suggesting recessive or X6-linked inheritance have also been described.
In addition to being associated with the genetic component, ethnicity has special emphasis when evaluated along with the phototypes of patients according to the Fitzpatrick scale9. As it is more frequent in blacks, Hispanics, and Asians, a possible relationship with the activity of melanocytes during the healing process can be traced.
Furthermore, the location of the keloid can directly affect its recurrence rate. Based on the current literature, systematic reviews and meta-analyses have shown high recurrence rates in the trunk region, up to three times higher than in the head and neck region, including ears, or even when compared to the limbs. Therefore, it is believed that the variation of skin tension forces in different body regions possibly generates these statistically significant differences10.
Despite its non-lethality, keloids impair mental and emotional quality of life, as demonstrated in recent studies, which is recovered after treatment11.
For its treatment, it is important to point out that exclusive excision, without association with an adjuvant method, has high recurrence rates, close to 50%, with an increase with each new attempt, especially in the first four years12.
Several studies have been trying to demonstrate the great importance of combining therapies, but still without a definitive result for this problem. New technologies are being associated with classic treatments, but also without showing maximum effectiveness13, 14.
Among the classic treatments, we can highlight the intralesional infiltration of drugs, such as corticosteroids and 5-fluoracil, in addition to the various adjuvant radiotherapy (RT) modalities: conventional RT, RT with an electron beam, RT in a single dose, and conventional X-ray15, 16.
Radiotherapy interferes with the formation of keloids by inhibiting the release of histamine by mast cells, reducing the proliferation of fibroblasts, and inhibiting TGF-Beta1, which suppresses collagen production17. External radiotherapy after surgical excision of keloids, proposed in the 1960s18, showed that alone it could alleviate the symptoms but failed to resolve the lesion when not associated with surgical excision. Furthermore, delay in performing radiotherapy after excision has been shown to result in higher recurrence rates.
However, radiotherapy with adjuvant in treating keloids raises great concern due to its carcinogenic potential. In 2009, a literature review found 5 cases that reported this occurrence. However, it was impossible to define whether adequate doses had been used in the reported cases and whether there was effective protection around the adjacent tissues19. Therefore, the conclusion is that the risk of carcinogenesis does not prevent the procedure from being performed, as long as care measures are taken for the surrounding tissues, which includes protection of the thyroid and mammary glands, especially in children and adolescents19.
Later, the possibility of treatment with internal or interstitial radiotherapy, known as brachytherapy, was introduced20. In this modality, there is a great capacity to focus the radiation on the target area, requiring a smaller dose and being more efficient, with less local radionecrosis and adverse effects on healthy tissues close to the keloid. However, there is still a higher hospital cost due to prolonged hospitalization and the use of specific and poorly available materials19.
A work carried out in Brazil highlighted the importance of RT with an electron beam; therefore, this possibility of treatment is maintained in the current approach routine for these lesions in our institution21, 22.
The keloid scar remains a medical challenge, both because of the difficult definition of the physiological factors that influence its formation and because of the need to associate therapies that, in some cases, do not cure or prevent the appearance of new lesions and recurrences.
OBJECTIVE
Therefore, this study aims to present a retrospective analysis of patients undergoing postoperative radiotherapy at the Hospital das Clínicas da Faculdade de Medicina de Botucatu over a four-year period to outline their epidemiological profile.
METHOD
Postoperative radiotherapy treatment protocol
Patients are referred to the Radiotherapy sector for clinical evaluation and scheduling the first photoelectron radiotherapy session using the Clinac 2100-C linear accelerator device (Varian-USA), with an energy of 4 million electron volts (Mev). 32Gray schemes divided into 16 sessions are programmed, 5 days a week. At the end of the 16 sessions, patients are reassessed for the need for booster doses of 8Gray in 4 sessions.
Radiotherapy was indicated for all referred patients who had undergone some previous therapy without success for treating keloids or recurrences and who were going to undergo keloid resection surgery.
The first session is always scheduled within 24 to 48 hours after keloid resection surgery in adults and children.
Analysis of medical records
Retrospective analysis of medical records to assess the profile of patients who underwent postoperative radiotherapy for the treatment of keloids at Hospital das Clínicas da Faculdade de Medicina de Botucatu (HC-FMB) from January 2015 to January 2019, whose data from the medical record allowed the inclusion in the study.
All female and male patients, adults, and children who underwent the treatment protocol of the Radiotherapy service at HC-FMB UNESP were included.
Patients whose medical records did not have confirmatory data on keloid scar treatment with surgery performed at the same hospital or an outpatient service and radiotherapy were excluded.
As it is a cross-sectional study, it was possible to apply the STROBE initiative partially (Strengthening the Reporting of Observational Studies in Epidemiology)23 to guide the review.
Researched variables - Epidemiological data
While analyzing medical records, we sought to determine the following variables: age, sex, education level, city of origin, race, cause of the scar, previous treatments, keloid site, treatment time, dose, and number of applications of radiotherapy.
Data collect
The data collection methodology used a form developed especially for this study (Appendix I), filled out by the researcher in the Department of Plastic Surgery, while evaluating the medical records of the patients included in the study. Data collection was carried out after approval by the Research Ethics Committee.
Analysis of data from medical records
These data were tabulated using Microsoft Excel® software to perform descriptive statistical analysis.
For qualitative variables, Pearson’s non-parametric chi-square test was performed, while, for the quantitative variables, analysis of variance was used to compare the different means and standard deviations related to the year of attendance and Student’s t-test to compare the means and standard deviations according to the patient’s gender.
The Kaplan-Meier estimator was also used to study the duration of treatment and its conclusion according to several variables (gender, specialty that made the referral for radiotherapy, city of origin, education, previous treatments, race, keloid etiology, and location).
The software used for statistical analysis was SAS version 9.2. The confidence interval was 95%, considering the p-value statistically significant when less than 0.05.
RESULTS
After reviewing medical records, we identified 27 people treated in 2015, 43 in 2016, 21 in 2017, and 40 in 2018, totaling 131 patients. Some had more than one irradiated lesion, with a total of 269 treated keloid scars.
Treatment duration ranged from 1 to 92 days after the first irradiation, averaging 51 days. The number of sessions was between 1 and 25, with a mean of 17. Table 1 shows the mean and standard deviation for the variables age, dose, number of applications, and treatment time in days according to the years evaluated, being that in 2018 and 2017, there were a greater number of sessions than in previous years.
| Year | P | ||||
|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | ||
| Age (in years) | 31.5 | 29.2 | 33.5 | 31.9 | 0.17 |
| 12.9 | 10.7 | 11.8 | 10.9 | ||
| Doses | 3164.0 | 3394.7 | 3668.2 | 3994.8 | <0.001 |
| 991.1 | 834.6 | 835.4 | 574.0 | ||
| Number of applications | 15.7 | 17.0 | 18.5 | 19.9 | <0.001 |
| 5.0 | 4.2 | 4.3 | 2.9 | ||
| Time (in days) | 36.1 | 37.4 | 46.1 | 56.2 | <0.001 |
| 19.6 | 17.7 | 16.2 | 17.7 | ||

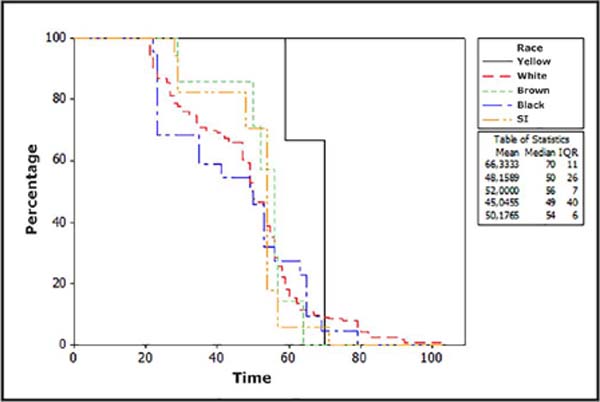
The majority of patients were white (78.8%), followed by black (10%), brown (3.7%), and yellow (1.1%). There was no distinction of race described in the medical records in 6.3% of the cases, in addition to not being possible to classify the patients according to the Fitzpatrick scale (Table 2).
| Year | Race | Total | ||||
|---|---|---|---|---|---|---|
| Yellow | White | Brown | Black | N/D | ||
| 2015 | - | 37 | 6 | two | 5 | 50 |
| 0.0 | 74% | 12% | 4% | 10% | 100 (%) | |
| 2016 | - | 70 | - | 6 | - | 76 |
| 0.0 | 92.1% | 0.0 | 7.9% | 0.0 | 100 (%) | |
| 2017 | - | 39 | 3 | 15 | 9 | 66 |
| 0.0 | 59.1% | 4.6% | 22.7% | 13.6% | 100 (%) | |
| 2018 | 3 | 66 | 1 | 4 | 3 | 77 |
| 3.9% | 85.7% | 1.3% | 5.2% | 3.9% | 100 (%) | |
| Total | 3 | 212 | 10 | 27 | 17 | 269 |
| 1.1% | 78.8% | 3.7% | 10% | 6.3% | 100 (%) | |

According to the Kaplan-Meier estimator, there was no difference between races in terms of whether or not they completed treatment with radiotherapy (Figure 1).

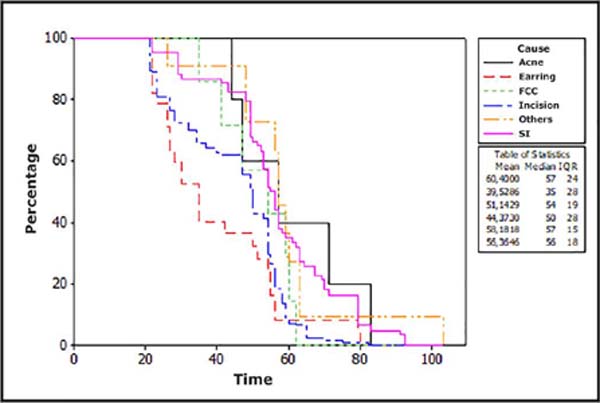
As causes of keloid formation, a surgical incision was described in 49% of the lesions, followed by earrings in 11%. There was no adequate information about the etiology of the lesion in 30% of the cases. Other causes with an incidence of less than 2% were, in descending order: trauma (blunt-cut injuries), acne, tumors, spontaneous appearance, bites, and folliculitis (Table 3). According to the Kaplan-Meier estimator (Figure 2), those patients with keloid scars secondary to acne or of undetermined cause tended to complete the treatment more than those caused by earrings and surgical incisions (p<0.0001).
| Cause | Year | Total | |||
|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | ||
| Acne | - | 1 | 2 | 2 | 5 |
| 0.0 | 1.3% | 3% | 2.6% | 1.9% | |
| Earring | 18 | 14 | - | - | 32 |
| 36% | 18.4% | 0.0 | 0.0 | 11.9% | |
| Spontaneous | - | - | - | 1 | 1 |
| 0.0 | 0.0 | 0.0 | 1.3% | 0.4% | |
| CBW | 2 | 4 | - | 1 | 7 |
| 4.0% | 5.3% | 0.0 | 1.3% | 2.6% | |
| Folliculitis | 0 | 1 | 1 | - | 2 |
| 0.0 | 1.3% | 1.5% | 0.0 | 0.7% | |
| Incision | 19 | 37 | 34 | 42 | 132 |
| 38% | 48.7% | 51.5% | 54.5% | 49.1% | |
| Bite | 2 | - | - | - | 2 |
| 4% | 0.0 | 0.0 | 0.0 | 0.7% | |
| Burn | 1 | 2 | - | - | 3 |
| 2% | 2.6% | 0.0 | 0.0 | 1.1% | |
| N/D | 6 | 17 | 27 | 31 | 81 |
| 12% | 22.4% | 40.9% | 40.3% | 30.1% | |
| Tumor | 1 | - | 2 | - | 3 |
| 2% | 0.0 | 3% | 0.0 | 1.1% | |
| Wart | 1 | - | - | - | 1 |
| 2% | 0.0 | 0.0 | 0.0 | 0.4% | |
| Total | 50 | 76 | 66 | 77 | 269 |

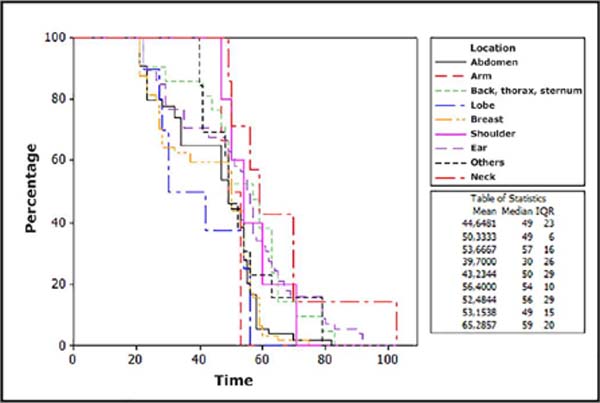
Several locations were identified, the most prevalent being the ears – including the lobe (33%), breasts (23%), and abdomen (22%). The other locations described were, in descending order: thorax, neck, inguinal region, sternum, arm, armpit, hand, thigh, leg, and lip (Table 4). Using the Kaplan-Meier estimator (Figure 3), we observed a greater chance of completing the treatment for those with injuries to the neck, back, and chest (including sternum) than those with injuries to the abdomen and earlobe (p<0.0001).
| Location | Year | Total | |||
|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | ||
| Abdomen | 11 | 14 | 21 | 15 | 61 |
| 22% | 18.4% | 31.8% | 19.5% | 22.7% | |
| Armpit | - | - | - | 2 | 2 |
| 0.0 | 0.0 | 0.0 | 2.6% | 0.7% | |
| Hip | - | - | - | 2 | 2 |
| 0.0 | 0.0 | 0.0 | 2.6% | 0.7% | |
| Arm | - | 5 | - | 1 | 6 |
| 0.0 | 6.6% | 0.0 | 1.3% | 2.2% | |
| Thigh | 1 | - | - | - | 1 |
| 2% | 0.0 | 0.0 | 0.0 | 0.4% | |
| Back | 1 | - | 2 | 2 | 5 |
| 2% | 0.0 | 3% | 2.6% | 1.9% | |
| Sternum | 2 | 1 | 2 | 1 | 6 |
| 4% | 1.3% | 3% | 1.3% | 2.2% | |
| Face | - | - | 3 | - | 3 |
| 0.0 | 0.0 | 4.5% | 0.0 | 1.1% | |
| Inguinal | 3 | - | - | - | 3 |
| 6% | 0.0 | 0.0 | 0.0 | 1.1% | |
| Lip | 1 | - | - | - | 1 |
| 2% | 0.0 | 0.0 | 0.0 | 0.4% | |
| Lobe | 12 | - | - | - | 12 |
| 24% | 0.0 | 0.0 | 0.0 | 4.5% | |
| Breast | 6 | 23 | 10 | 25 | 64 |
| 12% | 30.3% | 15.2% | 32.5% | 23.8% | |
| Hand | - | 1 | - | - | 1 |
| 0.0 | 1.3% | 0.0 | 0.0 | 0.4% | |
| Shoulder | 2 | 2 | - | 1 | 5 |
| 4% | 2.6% | 0.0 | 1.3% | 1.9% | |
| Ear | 10 | 24 | 20 | 22 | 76 |
| 20% | 31.6% | 30.3% | 28.6% | 28.3% | |
| Leg | - | 1 | - | - | 1 |
| 0.0 | 1.3% | 0.0 | 0.0 | 0.4% | |
| Neck | 1 | 2 | 3 | 3 | 9 |
| 2% | 2.6% | 4.5% | 3.9% | 3.3% | |
| Fist | - | - | 1 | - | 1 |
| 0.0 | 0.0 | 1.5% | 0.0 | 0.4% | |
| Chest | - | 3 | 4 | 3 | 10 |
| 0.0 | 3.9% | 6.1% | 3.9% | 3.7% | |
| Total | 50 | 76 | 66 | 77 | 269 |

Most injuries referred came from male and female plastic surgeons (63%), followed by Dermatology (12%), Head and Neck Surgery (3%), and Mastology (0.4%). In 20% of cases, there was no information on the specialty that referred the patient to the Radiotherapy sector.
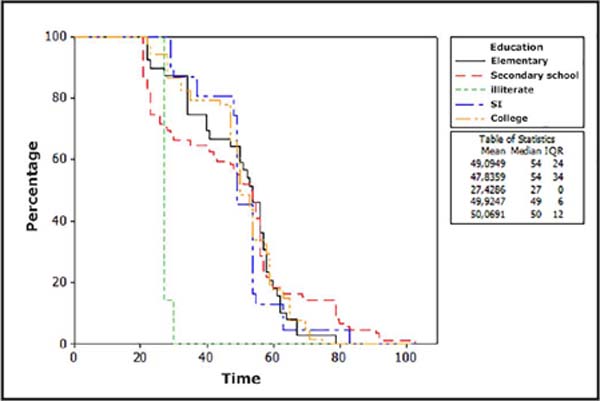
Regarding education, 38% completed or attended high school, 29% completed or were attending higher education, and 15% and 2% completed or attended elementary school II and I, respectively. In all, 3% of the patients were illiterate and in 11% of the cases this information was not available (Table 5). According to the Kaplan-Meier estimator (Figure 4), illiterate patients completed less treatment than those with complete elementary and middle classes (p<0.0001).
| Education | Year | Total | |||
|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | ||
| Elementary 1 | 1 | 1 | 3 | 1 | 6 |
| 2% | 1.3% | 4.6% | 1.3% | 2.2% | |
| Elementary 2 | 15 | 11 | 8 | 6 | 40 |
| 30% | 14.5% | 12.1% | 7.8% | 14.9% | |
| Average | 16 | 34 | 25 | 28 | 103 |
| 32% | 44.7% | 37.9% | 36.4% | 38.3% | |
| Illiterate | 1 | - | 2 | 6 | 9 |
| 2% | 0.0 | 3% | 7.8% | 3.4% | |
| N/D | 5 | 1 | 19 | 7 | 32 |
| 10% | 1.3% | 28.8% | 9.1% | 11.9% | |
| Higher | 12 | 29 | 9 | 29 | 79 |
| 24% | 38.2% | 13.6% | 37.7% | 29.4% | |
| Total | 50 | 76 | 66 | 77 | 269 |


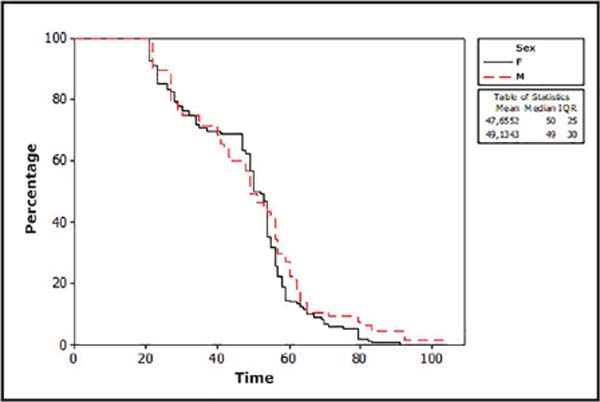
There was a predominance of women undergoing this treatment, corresponding to 70% of the treated lesions. Furthermore, we observed that women tend to complete more treatment than men (Table 6) in a statistically significant way (p=0.04). This finding is also confirmed when evaluating the number and volume of larger doses in women, with p-values of 0.03 and 0.02. The average age of women was also higher, being 34 years for women and 24 years for men. Using the Kaplan-Meier estimator to assess the relationship between sex and treatment time as factors for completing or not completing radiotherapy sessions, there was no statistically significant difference (Figure 5).


Another interesting assessment was that female patients had a higher mean age than men, with more radiation doses received and, therefore, a greater number of applications, but in a total treatment time similar to that of men (Table 7).
| Sex | P | ||
|---|---|---|---|
| Masculine | Feminine | ||
| Age (in years) | 24.9 | 34.2 | <0.0001 |
| 10.5 | 10.7 | ||
| Doses | 3417.5 | 3664.0 | 0.03 |
| 1030.8 | 759.4 | ||
| Number of applications | 17.0 | 18.3 | 0.02 |
| 5.2 | 3.9 | ||
| Time (in days) | 43.6 | 45.2 | 0.56 |
| 22.3 | 18.1 | ||

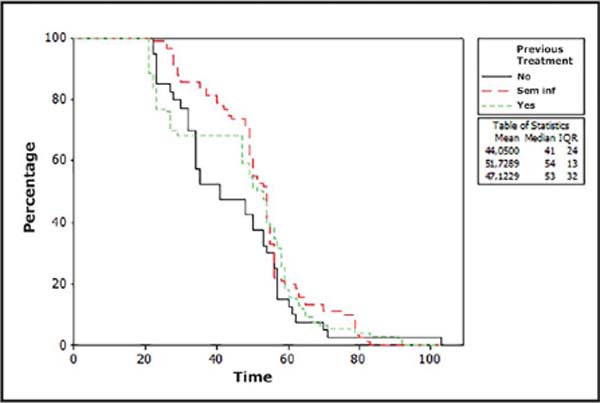
In 43% of the lesions, some previous treatment had already been tried without success; in 41% of the cases, this was impossible to determine. Using the Kaplan-Meier estimator, no statistical difference was observed for completing the radiotherapy scheme in those who had or had not previously undergone other treatments. (Figure 6).

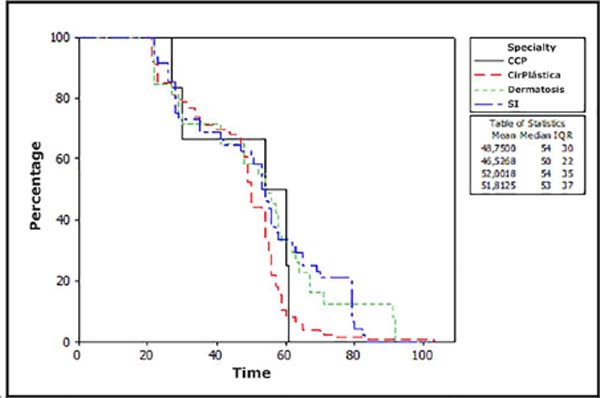
According to the Kaplan-Meier estimator (Figure 7), patients referred by the Dermatology and Head and Neck Surgery specialties tended to complete more treatment than those referred by Plastic Surgery (p=0.002).

DISCUSSION
Keloids, being benign alteration, can easily have their treatment neglected for several reasons. Therefore, we consider it essential that the doctor who conducts this type of treatment, in addition to knowing the available techniques, also knows how to identify and guide their patients about the evolution of the treatment and the importance of completing it, especially because it has high rates of relapse when not done properly.
From the analysis of the medical records, we observed some findings that can guide our attention during the consultations to achieve better results for the patients.
Some studies demonstrate a higher prevalence and incidence of keloids in the black population of African origin24; however, in our review, we observed a greater predominance of patients declared to be white. This may be related to the historical and social fact that in Brazil, blacks have their health neglected, not seeking health services to treat benign conditions.
It is also necessary to consider the great miscegenation of the Brazilian population, which means that many declared white patients have African roots. The Botucatu region is predominantly colonized by Europeans, which may also interfere with these data. Fortunately, the racial factor was not decisive for the patient to complete or not the treatment.
The scar’s location suggests that it is related to the formation of keloids since the areas that suffer the most stretching or elongation have a higher frequency of pathological scars25. Our study observed their higher prevalence in the ears, breasts, and abdomen. Other body regions, such as the face and scalp, were less frequent or absent. These data are similar to the literature26. Furthermore, there was a greater chance of completing the treatment for neck, back and chest injuries than for abdomen and earlobe injuries. Thus, it was unclear whether exposed areas influenced prolonged treatment commitment.
We noted that the causes of keloid formation were predominantly from surgical incisions, with almost half of the cases followed by earrings. Such patients tended to complete less treatment compared to those with keloid scars secondary to acne or of undetermined cause, with statistical significance.
Another interesting fact was that illiterate patients completed less treatment than those with complete primary and secondary education, which indicates an influence of schooling on adherence to complete treatment.
We observed that the average age of the patients was between 24 and 34 years old, characterizing a young and economically active population, that is, people who are inserted in the labor market and will miss many working days of service during treatment, which has an average of 43 to 45 days. This can have a major negative impact on the completion of treatment, favoring relapses over time.
Some studies show a predominance of keloids in women, with a possible relationship with estrogen levels27. There are many reports of worsening symptoms during pregnancy, for example. In our analysis, women sought the health service more than men, which justifies their great predominance, more than two-thirds, in the total number of cases; in addition, female patients tended to complete more treatment than males.
Furthermore, women were older on average than men, receiving higher numbers of radiation doses performed in more applications; however, the total treatment time was similar, which may suggest that male patients are attending on dates outside the deadline, lengthening the time, but without completing it properly. These data align with what we know about men seeking fewer health services28 and being less adherent to the proposed treatments.
When reviewing the medical literature, we observed that there are many ways described for treating keloid scars. Due to the great challenge of the definitive and effective treatment of this pathological scar, new therapeutic modalities and combinations of previous treatments are constantly emerging.
Radiotherapy reduces the action of fibroblasts on keloids in a dose-dependent manner29. Currently, after its great evolution in the 20th century, it presents itself in two main forms: internal and external. Brachytherapy is studied as an internal option, while electron beams and X-rays are the most common external application forms. Although some studies indicate the superiority of brachytherapy in preventing keloid recurrence30, many meta-analyses have not been able to confirm this in a statistically significant way13.
By associating surgical excision with early radiotherapy, superior results were found11.
It is important to emphasize that the adverse signs and symptoms of radiotherapy are similar to those of corticoids, involving erythema, desquamation, and depigmentation; however, the complaint of pain is not frequent19. In our review, we could not properly identify these complaints due to the descriptions not clearly reporting whether or not there were such complaints.
As a limitation of this study, it was impossible to assess the current rate of HC-FMB recurrence with the proposed therapies and clinically reassess the patients who had their data reviewed in the medical records.
CONCLUSION
Postoperative radiotherapy on keloids is a treatment enshrined in the medical literature and an important tool for plastic surgeons who manage these pathological scars. Treatment is usually long-term and should be started early after surgery, requiring patient commitment to achieve the best results.
There was a predominance of women and white patients seeking and receiving the complete treatment, while people with low education could not adequately complete the treatment, and may have lower therapeutic success rates.
Therefore, changing the approach to patients with less education and those who are male will help improve adherence and short- and long-term outcomes for these patients.
1. Hospital das Clínicas da Faculdade de Medicina de Botucatu, Cirurgia Plástica,
Botucatu, SP, Brazil.
2. Hospital das Clínicas da Faculdade de Medicina de Botucatu, Radioterapia, Botucatu,
SP, Brazil.
Corresponding author: Balduino Ferreira de Menezes-Neto Unesp - Pronto Socorro Rua Doutor Adolfo Pardini Filho, 1028, Chácara Recreio Vista Alegre, Botucatu, SP, Brazil. CEP: 18608-760E-mail: balduinofmneto@gmail.com
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket