



Original Article - Year 2023 - Volume 38 -
Simplified vacuum dressing system: operational and financial feasibility study in the management of wounds
Curativo a vácuo simplificado: estudo de viabilidade operacional e financeira no tratamento de feridas
Sandro Cilindro de Souza1* ; Carlos Maurício Cardeal Mendes1; Jose Valber Lima Meneses1; Rosana dias Menezes2
; Carlos Maurício Cardeal Mendes1; Jose Valber Lima Meneses1; Rosana dias Menezes2
ABSTRACT
Introduction: The high cost of negative pressure wound therapy (NPWT) makes the procedure less accessible in institutions with limited resources. To solve the problem, streamlined vacuum dressings have been proposed, but the usefulness of these devices has been poorly studied. The objective of this work is to evaluate the feasibility (operational and financial) of a simplified vacuum dressing system model (SVDM).
Methods: Operational viability was assessed by studying application time and quantity of dressings performed; financial viability, by analyzing the economic costs of dressing changes.
Results: Fifty wounds were treated (25 in each group: SVDM x silver hydrofiber). For SVDM, the number of dressings per patient was lower, while the application time was higher. The SVDM showed higher costs. The increase in the expenses associated with the SVDM was related to the average selling price of the product and the number of dressing changes; treatment time and application time of the SVDM did not interfere with costs. In contrast, SVDM costs proved to be below the announced expenses for conventional NPWT.
Conclusion: SVDM was considered viable as long as qualified teams perform it and results in few dressing changes (< 3).
Keywords: Reconstructive surgical procedures; Wounds and injuries; Negativepressure wound therapy; Costs and cost analysis; Wound healing
RESUMO
Introdução: O alto custo da terapia de pressão negativa (TPN) torna o procedimento menos
acessível em instituições com recursos limitados. Para resolver o problema,
têm sido propostos os curativos a vácuo simplificados, mas a utilidade
desses equipamentos ainda é pouco estudada. O objetivo desse trabalho é
avaliar a viabilidade (operacional e financeira) de um modelo de curativo a
vácuo simplificado (MCVS).
Método: A viabilidade operacional foi avaliada por meio de estudo de tempo de
instalação e quantidade de curativos realizados; a financeira, por análise
de custos econômicos de trocas de curativos.
Resultados: Foram tratadas 50 feridas (25 em cada grupo: MCVS x hidrofibra prata). Para o
MCVS, o número de curativos por paciente foi menor, enquanto o tempo de
instalação, maior. MCVS apresentou custos maiores. O aumento de custo
associado a MCVS foi relacionado ao preço médio de comercialização do
produto e quantidade de trocas de curativos; tempo de tratamento e tempo de
instalação do MCVS não interferiram em custos. Em contraste, os custos do
MCVS se mostraram bem inferiores aos custos anunciados para a TPN
convencional.
Conclusão: MCVS foi considerado viável desde que seja feito por equipes qualificadas e
resulte em poucas trocas de curativos (< 3).
Palavras-chave: Procedimentos cirúrgicos reconstrutivos; Ferimentos e lesões; Tratamento de ferimentos com pressão negativa; Custos e análise de custo; Cicatrização
INTRODUCTION
Since its introduction two decades ago1,2, negative pressure wound therapy (NPWT) has been established for its effectiveness in managing acute and chronic wounds3-7. However, the high technology makes the device complex to handle and expensive, reducing its use in institutions with limited resources8. Trying to solve these problems, simplified vacuum dressings systems (SVD)8-12 have been proposed since NPWT does not necessarily require a special apparatus and can prepare wounds for surgical treatment8,12-14. Despite using more basic mechanical and electrical components, SVD retains essential safety attributes such as controlled suction and wound sealing1,8,10,15,16.
Operational characteristics of SVD have been poorly evaluated and, occasionally, seriously criticized3,16. Most of the studies available do not have comparison groups and use limited methodologies, thus deserving further evaluation8,10,11,15,17,18. The primary deficiencies are the use of rudimentary materials, difficulty sealing wounds, and inability to maintain subatmospheric pressures8,15,16,19. Deficiencies result in accumulations of exudates, dressing changes, and repeated manipulation of injuries. In addition to being boring, manipulations increase the risk of aggravating injuries. In minor exudative wounds, inadequate seals can cause perilesional air circulation, resulting in dryness, hemorrhage, and progressive tissue necrosis1,19-21.
The decision to use a specific dressing should be guided not only by potential efficacy, adverse effects, location, and symptoms of lesions (pain, exudate, etc.) but also by the frequency of changes, clinical experience, patient preference, and costs22-24. Even when economic value is not an issue, the best treatment may be challenging to implement or unavailable, so it is essential to know efficient second indication alternatives22.
OBJECTIVE
The study’s objective was to evaluate the feasibility (operational and financial) of an SVD model (SVDM).
MATERIAL AND METHODS
Feasibility study based on a randomized superiority clinical trial, blinded, with two parallel arms, carried out between January 1, 2017, and May 1, 2020, Roberto Santos Hospital (RSH; teaching hospital, multidisciplinary, 640 beds - Salvador, Bahia - Brazil). The trial was registered in the Brazilian Registry of Clinical Trials (RBR-5c8y6v) and followed CONSORT 2010 recommendations25. The research was approved by the Research Ethics Council of the RSH (CAAE 55556816.7.0000.5028) and performed following the Declaration of Helsinki. An Informed Consent Form was obtained from the participating patients.
A sample of 50 patients was calculated using the R statistical software (R Core Team, 2018), assuming a mean expected success rate of 98% for the SVDM group and 72% for the control group, with a margin of superiority of 25%. A test power of 80% and a significance level of 5% were assumed. Patients were admitted sequentially in treatment (SVDM) and control groups (hydrofiber silver - SHF, Aquacel Ag+ Extra™ - Convatec Inc., ER Squibb & Sons, North Carolina - USA) following a list of random numbers performed in the statistical software R. The statistical analysis used was by treatment protocol.
Adult patients hospitalized for acute (< 3 months) or chronic (≥ 3 months) wounds were included in the study. Subjects with decompensated systemic disorders (cardiac, thyroid, renal, pulmonary, hepatic, arterial hypertension, severe anemia, severe malnutrition, and coagulopathies) were excluded. Painful wounds, infected wounds, injuries associated with perilesional dermatoses, allergic reactions, malignant neoplasms, and exposure to underlying exposed vessels, nerves, or viscera were also not included. The emergence of serious complications (e.g., hemorrhage, allergic reactions, sepsis, extensive necrosis, severe pain), decompensation of previously controlled systemic disorders, and deaths not attributable to the dressings were exclusion criteria used.
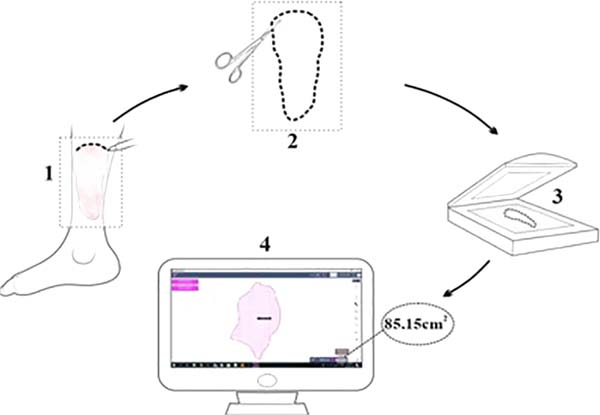
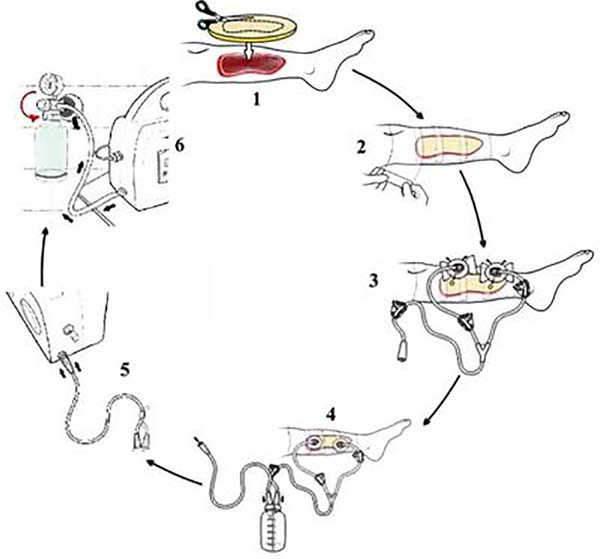
Wounded areas were obtained using the SketchandCalc app (www.sketchandcalc.com - Figure 1). Application, SVDM, and clinical examples are shown in Figures 2 to 4. SVDM was regulated with a pressure of -125 mmHg. The first dressing was used in continuous mode and the others in intermittent mode (5 minutes of vacuum and 2 minutes without vacuum)2,26.





In both groups, debridements were performed to remove devitalized tissue occasionally present. Changes were made at ≥ 50% saturation of dressings to avoid unpleasant odor27. Patients were followed for 14 days or until the granular lesion (≥ 75% of the raw bed covered by healthy-looking granulation tissue).
The operational (ease of application and use) and financial feasibility (cost of dressing changes) of the SVDM were evaluated. For operational feasibility, outcomes analyzed were application time and amount of dressings; for financial viability, total economic costs, and cost of dressing changes. Due to the asymmetry of study variables, statistical analyses were performed using the median, interquartile range, and bivariate standardized difference to compare types of dressings.
Difference qualification criteria standardized were: [0-0.2]: absent; (0.2-0.5]: small; (0.5-0.8]: moderate; [>0.8]: large (Cohen, 1988). P-values calculated from the same test were adjusted for four multiple comparisons under dependence conditions by the Benjamini & Yekutieli method28. For cost estimates adjusted for dressing application time, number of dressings, and treatment time, the robust regression model was used with τ = 0.5 (median)29. An overall α error of 0.05 was assumed for the entire study.
RESULTS
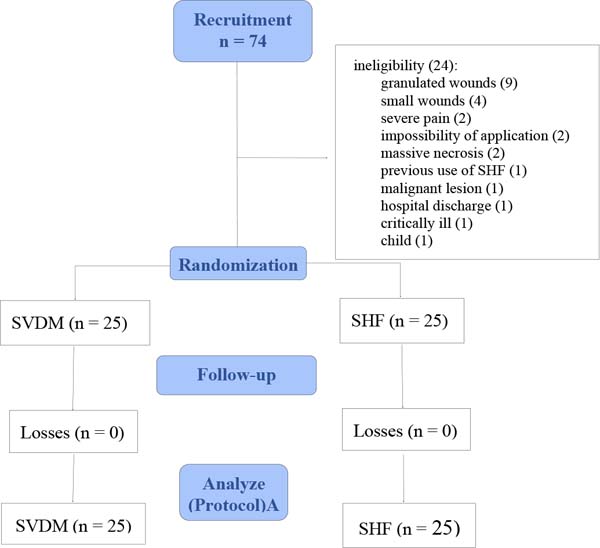
Of the 74 inpatients evaluated, 24 were excluded because they did not meet the inclusion criteria (Figure 5). Patients studied were mainly men (SVDM: 52% x SHF: 68%), mixed race (SVDM: 72% x SHF: 84%), non-obese (88%, both groups), and mean age in the age group 6th decade (SVDM: 55 years x SHF: 50 years -Table 1). Adding the results of both groups, 270 dressings were applied in 589 days of treatment.
| Variable | SVDM (n = 25) | SHF (n = 25) | ||
|---|---|---|---|---|
| Mean (SD) (CV%) | Min/Max | Mean (SD) (CV%) | Min/Max | |
| Age (years) | 55 (14) (25) | 29/85 | 50 (16) (32) | 15/79 |
| Weight (Kg) | 67 (16) (23.9) | 47/108 | 68 (15) (21.8) | 43/103 |
| Height (cm) | 164 (11) (6.9) | 145/184 | 166 (12) (6.9) | 154/180 |
| n | % | n | % | |
| Sex | ||||
| Men | 13 | 52 | 17 | 68 |
| Women | 12 | 48 | 8 | 32 |
| Ethnicity | ||||
| Brown | 18 | 72 | 21 | 84 |
| Black | 5 | 20 | 2 | 8 |
| White | 2 | 8 | 2 | 8 |
| BMI | ||||
| Low weight | 2 | 8 | 3 | 12 |
| Normal | 10 | 40 | 11 | 44 |
| Overweight | 10 | 40 | 8 | 32 |
| Obesity | 3 | 12 | 3 | 12 |
SD: standard deviation; CV%: coefficient of percentage variation; BMI: body mass index (Kg/cm2); Max.: maximum; Min.: Minimum.


The median application time of the simplified dressing, in minutes, was about 6 times greater than that of SHF (22,7 min x 4,0 min; Sd=0.84; p=0.0008). SVDM group showed a difference, for less, of 4 days of treatment (3 days x 7 days; Sd=0.57; p=0.0028) and of 4 dressing changes (3 dressings x 7 dressings; Sd = 0.85; p<0.0027) (Table 2).
| Variable | SVDM (n = 25) | SHF (n= 25) | ||||||
|---|---|---|---|---|---|---|---|---|
| Md(IIQ R) | Min/Max | CVMd% | Md(IIQR) | Min/Max | CVMd% | Sd | p* | |
| Installation time of dressing (min) |
22.71 (10.0) | 16.5/38.7 | 44.0 | 4.0(3.0) | 2.2/10.4 | 75.6 | 0.84 | 0.0008 |
| Treatment time (days) | 10(5) | 3/15 | 50.0 | 14(0) | 7/15 | 0.0 | 0.57 | 0.0028 |
| Dressings/patient | 3(1) | 1/4 | 33.3 | 7(2) | 6/14 | 28.6 | 0.85 | 0.0027 |
Max: maximum; Min: Minimum; Md(IIQ): median (interquartile range); CVMd%: coefficient of variation percentage of the median; Sd: standardized difference (measure of statistical association): Cohen’s criterion30 for Sd: [0-0.2]: absent; (0.2-0.5]: small; (0.5-0.8]: moderate; >0.8: large;
* adjusted p-value for multiple comparisons under dependency relationships28.

Table 3 (financial feasibility) presents cost estimates adjusted for application time per dressing, number of dressings, and treatment time using a robust regression model with τ = 0.5 (median). In the raw model (which only contains the type of dressing as an independent variable), it is observed that the difference in predicted cost of SVDM to SHF was only US$ 5.88. However, when adding other variables mentioned (covariates), the difference became US$ 209.99 (adjusted model 1). There was, therefore, a significant change when considering all covariates; thus, the crude model proved unsatisfactory for predicting the median cost difference between dressings.
| Variable | Gross model |
Adjusted model 1 |
Adjusted model 2 |
Saturated model |
Final adjusted model | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cost (R$) | pB | Cost (R$) | pAj1 | VIF | Cost (R$) | pAj2 | Cost (R$) | pS | Cost (R$) | pAjf | |
| Intercept (β0) | 931.26 | < 0.0001 |
-1139.05 | < 0.0001 | - | -1269.37 | < 0.0001 | -894.75 | 0.1960 | -1270.55 | < 0.0001 |
| SVDM (β1) | -31.19 | 0.8470 | 1112.96 | 0.0001 | 2.10 | 1275.15 | < 0.0001 | 890.53 | 0.1978 | 1282.82 | < 0.0001 |
| Installation time per dressing (min) (β2) | - | - | 0.74 | 0.7080 | 2.52 | 0.31 | 0.9138 | - | - | - | - |
| Number of dressings (β3) | - | - | 246.00 | 0.0017 | 55.89 | 297.17 | < 0.0001 | 245.92 | 0.0137 | 297.48 | < 0.0001 |
| Treatment time (days) (β4) | - | - | 17.03 | 0.4032 | 47.72 | - | - | - | - | - | - |
| SVDM
(β1) x Number of dressings (β3) |
- | - | - | - | - | - | - | 58.20 | 0.5462 | - | - |
Cost: predicted median cost; pB: raw model p-value; pAj1: p-value of the adjusted model 1; VIF: variance inflation factor - acceptable VIF: ≥ 10; pAj2: p-value of the adjusted model 2; pS: p-value of the final adjusted model.

Adjusted model 1 showed a strong correlation (multicollinearity) between the number of dressings and the treatment time, with variance inflation factor (VIF) values greater than ten31. Therefore, these covariates cannot remain together in the model to avoid bias. As the number of dressings was the covariate that showed the most remarkable difference in cost, the covariate, the treatment time was excluded from the model.
In adjusted model 2, the application time covariate did not contribute to the predicted cost (US$ 0.31; p = 0.9138), being removed from the model.
In adjusted model 2, covariates that contributed to median cost estimates were the type of dressing and the number of dressings. However, their probable absence was evidenced after evaluating the interaction between these covariates in a saturated model with an interaction term (p=0.5462).
The final adjusted model shows that the estimated cost difference between SVDM and SHF was US$ 242.04 (p<0.0001). In other words, costs would be much higher for SVDM if the group required the same number of dressings as SHF. Since more SHF dressings were changed (SHF: 7 x SVDM: 3), both the cost difference found directly in the study (continuous lines) and the difference if the groups had the same number of dressings (dashed line) were represented in Figure 6.
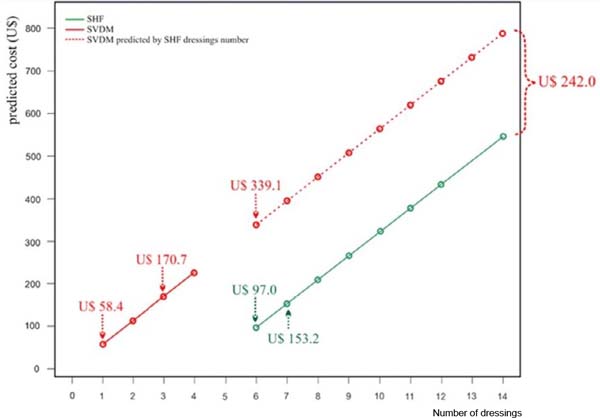
The figure shows, for example, that the estimated costs for six dressings (minimum number of dressings performed in the SHF group) were: SVDM: US$ 339.09 x SHF: US$ 97.04; estimated costs for the median number of dressings served in each group were SVDM (3 dressings): US$ 170.70 x SHF (7 dressings): US$ 153.17 (i.e., US$ 17.53 more per patient); finally, the estimated cost for 1 SVDM was US$ 58.44, which corresponds to an estimated price for 5.31 SHF. Therefore, the SVDM estimated cost was higher than the SHF estimated cost in all items evaluated.
DISCUSSION
SVD reduces technological resources to facilitate handling and minimize costs. However, simplification must not compromise product reliability8,11,16. To ensure safety, it is recommended that any NPTW equipment has suction control mechanisms to avoid extreme variations in subatmospheric pressure and, in cases of intense pressure, to prevent exsanguination through treated wounds3.
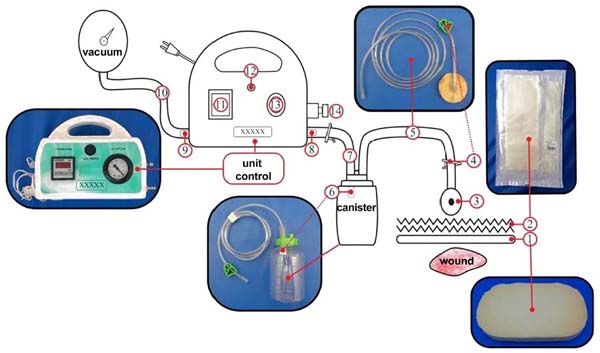
SVDM, in addition to containing these safety elements, including a pneumatic pressure gauge, was equipped with a small specialized filter (high molecular weight polyethylene - Figure 3) that becomes impervious when coming into contact with exudates, ensuring blockage of effluxes beyond the liquid collection canister. Finally, light-colored foams were used to facilitate observation of their degree of saturation and retention of debris. Conventional NPWT uses black foams, which makes this observation impossible. The transparency of a dressing allows continuous monitoring of wound beds and perilesional skin without violating the dressing, reducing changes and costs32.
Few data are available on handling vacuum dressings, making satisfactory discussions difficult. In a systematic review, the application method was briefly described without illustrations26. In line with the current monograph, a comparative study of chronic wound treatment using a wall suction SVD also reported six steps for applying the vacuum dressing13. Except for these papers and what is recorded in the conventional NPWT manufacturing manual, descriptions of placement steps have not been made in reviews on the subject3,4,33.
The longer application time SVDM (22.7 min x 3.98 min) was attributed to the greater complexity of using the device and, therefore, the need for training to master the procedure. The complexity was due to the multiple steps required for placement of the SVDM (6 steps x 2 steps), the increased care needed for sealing dressings (Figure 2, step 2), and the extra time required to remove foams adhered to wounds.
Only one randomized trial using an SVD model (also powered by the hospital vacuum) provided results in the references consulted, with an average application time of 19 min34. Compared with the present study, the difference of just under four minutes for dressing changes (22.71 min x 19 min) was considered clinically unimportant. The data suggests that the application complexity of the SVDM may be similar to that of other simplified dressing models.
Application complexity is also a problem related to conventional NPWT1,3,6, especially in wounds located in contoured areas (e.g., neck, hands, and feet), in places with recesses (e.g., between fingers, intergluteal crease), in regions that have natural orifices (e.g., perineum) or when perilesional skin is continuously moist (dermatoses, dermabrasions, burns, avulsions, among other conditions)1,3,6,13,35. The complexity is so significant that conventional NPWT is performed by highly trained nursing teams who do not work in the hospital that hires them, making it difficult for this team to access, especially at night, on weekends, in intensive care units, and operating rooms. Furthermore, obtaining and maintaining wound seals can be a frustrating exercise, further diminishing the popularity of vacuum dressings36. In contrast, occlusive dressings such as SHF are simple, direct, and quick to apply24. Finally, NPWT requires the additional work of daily face-to-face monitoring to prevent leaks13,14.
The SVDM maintained wound seals, controlled subatmospheric pressure, and drained exudates without early exchanges. As a result, maintenance of the SVDM (3 days) was similar to that described for most of both standard NPWT or other SVD (2 to 3 days)6,14,37. Vacuum dressings can be fully functional until ten days if the adhesive film is kept intact13,38. There was a reduction in the number of dressings in the SVDM group (3 x 7), attributed to the continuous drainage of fluids, which kept dressings unsaturated and operating longer8. Foams used in NPWT, thanks to their absorbent properties, allow fewer exchanges. To avoid making them smelly or adhesive, the dressings should be changed every two to three days39,40.
Accumulation of liquid during intermittency can break the film and result in leaks; consequently, intermittent NPWT has been replaced by a “variable NPWT,” characterized by a smooth cycle of variation between less intense pressures (-80 mmHg and -10mmHg) to maintain a continuous subatmospheric environment41,42. SVD powered by wall suction, such as the SVDM, may be desirable, as pressure variations in the hospital network (which are transmitted to the equipment) mimic the effects of variable NPWT.
Costs analysis is challenging, as available data are poor26 and, contrary to what was performed in the present trial, described without adjustments for covariates. SVDM costs depended on the average selling price (SVDM unit: US$ 56.6 x SHF unit 15 cm x 15 cm: US$ 20.5), the number of changes, and the type of dressing.
Results indicate that SVDM implies increased costs per patient (US$ 17.5 more) and per dressing change, with a single SVDM change (US$ 58.5) equivalent to the approximate cost of 5 SHF changes. However, four dressings are saved when opting for SVDM. Suppose the number of SVDM exchanges is similar to that of SHF exchanges; the cost difference increases (US$ 242.0 - Table 3, Figure 6). Therefore, care to ensure operational quality is essential so that the median number of SVDM dressing changes is not exceeded (three shifts); otherwise, the result would be a considerable increase in the final cost.
Direct costs obtained for SVDM appear much lower than for standard NPWT. The cost of conventional NPWT was estimated to range from US$ 1,750.0 to US$ 3,450.0 weekly and US$ 1,286.0 to US$ 5,452.0 per patient10,12,26,43. In children, the monthly cost of vacuum therapy was recently estimated at US$ 1,677/patient44. Treatment can become up to 20 times cheaper with simplified dressings systems than conventional NPWT10,45. SVD costs can be as low as US$ 6.4/dressing39, US$ 15.0/day14, or 2% of the average cost of using the VAC System12.
One reason for lower costs is that hospital vacuum systems, dispensing specialized devices10, supply SVD. Another reason is using simple, lower-cost, locally manufactured materials (foams, polyurethane films, canisters, tubes made of PVC plastic, etc.)11. Finally, the current study showed that the cost of SVDM can become even lower if the number of dressings per patient is minimized. The reduction in exchanges is possible, as fully functioning NPWT dressings for up to ten days have been described13,38.
CONCLUSION
SVDM proved greater operational complexity and cost, but it can be feasible as long professionals for the application master the procedure and there are no more than three dressing changes per patient.
1. Universidade Federal da Bahia, Salvador, BA,
Brazil
2. Secretaria de Saúde do Estado da Bahia,
Salvador, BA, Brazil
Corresponding author: Sandro Cilindro de Souza Av. Reitor Miguel Calmon, sala 110, 1º andar, Vale do Canela, Salvador, BA, Brazil., Zip Code: 40110-902, E-mail: sandrocilin@gmail.com
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket