



Articles - Year 2001 - Volume 16 -
Pharyngoesophageal Reconstruction: Using Microsurgical Jejunum and Pectoralis Major Flaps
Reconstrução Faringoesofágica: Utilização do Retalho Peitoral Maior e Jejuno Microcirúrgico
ABSTRACT
Pharyngoesophageal reconstruction is one of the major challenges of neck surgery. Many treatment options have been described. All of them involve procedures of greater or lesser technical complexity and high rates of complications and mortality. The present study describes the techniques performed at the Service of Plastic Surgery of the PUC-RS São Lucas Hospital in 10 reconstructions: myocutaneous pectoralis major flap and microsurgical jejunal flap. Indications, complications, advantages and disadvantages of each method are discussed.
Keywords: Pharyngoesophageal reconstruction; microsurgical jejunum and pectoralis major flap; free jejunum; cervical reconstruction
RESUMO
A reconstrução faringoesofágica é um dos maiores desafios cirúrgicos da região cervical. Existem diversas opções terapêuticas descritas. Todas envolvem procedimentos de maior ou menor grau de complexidade técnica e altas taxas de complicações e de mortalidade. Este artigo descreve as técnicas utilizadas no Serviço de Cirurgia Plástica do Hospital São Lucas da PUC-RS em 10 reconstruções: o retalho miocutâneo peitoral maior e o retalho microcirúrgico de jejuno. São discutidas as indicações, complicações, vantagens e desvantagens de cada método.
Palavras-chave: Reconstrução faringoesofágica; retalho peitoral maior e jejuno microcirúrgico; jejuno livre; reconstrução cervical
Malignant cervical tumors make up approximately 4% of all malignant tumors, of which epidermoid is the most frequent. These lesions are related to smoking and alcohol abuse(1) in men over 50 years of age. The main treatment is surgical resection that may be supplemented with radiotherapy and neoadjuvant chemotherapy. The most used reconstruction possibilities are jejunal, colon, stomach interposition, myocutaneous flaps of pectoralis major and fasciocutaneous flaps of the deltopectoral, cervical, antebrachial and lateral thigh regions.
We performed 10 pharyngoesophageal reconstructions in extensive circumferential defects, using microsurgical jejunal and pectoralis major flaps in our service.
The aim of the present study is to present two cervical esophageal and pharynx reconstruction techniques using a microsurgical jejunal loop and myocutaneous pectoralis major flap, their advantages, disadvantages, and discuss their indications and complications.
SURGICAL TECHNIQUE
PECTORALIS MAJOR MYOCUTANEOUS FLAP
A square with a size proportional to the pharyngoesophageal loss is designed over the pectoralis. A flap incision of the skin and muscle is made, detaching it from the sternum and ribs in the cranial direction, forming a myocutaneous flap supplied by the thoracic branch of the thoracoacromial artery and comitant veins, and lateral pectoralis nerve.
The flap may be taken to the cervical region by infra or supraclavicular routes . The flap is then tubulized, suturing its borders after the cervical region is reached. Then, proximal and distal anastomoses are performed. The muscle is fixed to cervical structures. Aspiration drains are positioned and the area is covered with cervical or neighboring flaps. The pectoral region is closed primarily or with a skin graft: (Figs. 1 & 2) .
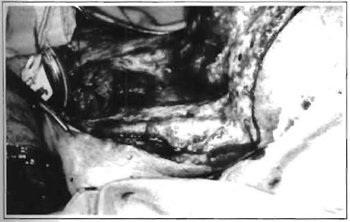
Fig. 1 - Cervical region prepared to receive a pectoralis major flap. The pharyngeal and esophageal stumps are evident.
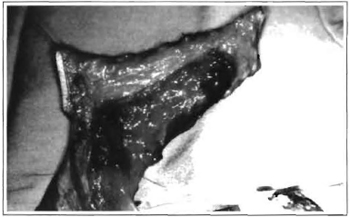
Fig. 2 -Myocutaneous flap of the tubulized pectoralis major.
JEJUNAL MICROSURGICAL FLAP
By means of a median supra-umbilical incision, a 15-20 cm jejunal segment is identified and resected, 45 to 60 cm from the Treitz angle(2,3), with a single vascular arch verified by transillumination(2,3,4). The enteroanastomosis is performed and the abdomen closed. The artery and receptor veins of the cervical region are repaired. We perform esophageal anastomosis to fix the flap before microsurgical anastomosis. Arterial and venous microanastomoses are performed, in this order, in the isoperistaltic position. Afterwards, pharyngeal anastomosis is performed. Closed-system aspiration drains are put on the neck. Skin coverage is performed with local cutaneous, myocutaneous flaps or skin grafts(2) (Figs. 3 & 4).

Fig. 3 -Jejunum loop prepared for interposition, with a limited vascular arch.
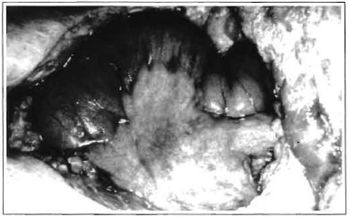
Fig. 4 -View of the viability of the jejunal loop maintained only by the pedicle.
POST-OPERATIVE PERIOD AND COMPLICATIONS
Post-operative care consists of cervical rest, a high bedpost, drain inspection, and tracheostomy care. A diluted barium pharingoesophagusgram is requested 15 days after surgery. Feeding starts with a nasoenteral tube on the 1st and 3rd PO days, for pectoralis and jejunum, respectively. We use prophylactic antibiotics for 24 hours (cefalotine). Graft viability is monitored by the patient's clinical follow-up and general health status.
The most common complications are salivary fistula (80% in some series)(2,3,4), flap stenosis, necrosis and infection.
DISCUSSION
Procedures involving prostheses, local grafts, cervical flaps have been used but were abandoned due to major complication rates. The deltopectoralis flap is still used, but also has a greater complication rate and requires a larger period of hospitalization. Since abdominal visceral interposition (stomach, colon) presents higher morbidity; it is used only for selected cases (for example: total esophagectomy, caustic esophagitis)(2) .
The antebrachial flap has also been performed by some authors, with satisfactory results(5).
The advantages of the jejunal flap are: greater anatomical similarity with the digestive tract, better esthetic results, smaller incidence of stenoses and fistulas, and it does not limit cervical emptying. The disadvantages are: need of laparotomy, enterectomy, larger surgical time.
We perform flap anastomosis with the esophagus before the vascular anastomoses aiming to attain better flap stability, which is important for the microsurgical procedure. We do not use systemic or local drugs at any time of the reconstruction.
The advantages of the myocutaneous pectoralis flap are: no laparotomy, optimal blood supply and better mediastinum filling(6). Better vocal recovery has been observed with skin coverage flaps compared to those with mucosa(5). The disadvantages are: higher incidence of stenoses and fistulas, need of larger esophageal stumps and less tube lubrication. The time for reintroducing feeding is controversial; it may be early (1st day) or late (7th, 10th or 12th day) (2,3,7). For pectoralis major, we begin nasoenteral tube feeding on the 1st post-operative day; for jejunum, after the recovery of intestinal peristalsis, around the 3rd day.
We perform a contrast X-ray at least 15 days after surgery and, if good permeability and no fistulas are observed, we remove the tube, progressively introducing water, liquid and semi-liquid diet, according to acceptance. We assess the viability of grafts by the patient's health status and by the local exam of the cervical region (Figs. 5-8).

Fig. 5 - 30th PO day -Pectoralis major flap. No fistulas and adequate flow in the contrast X-ray.
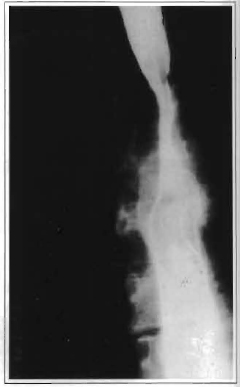
Fig. 6 -A lower view of the exam.
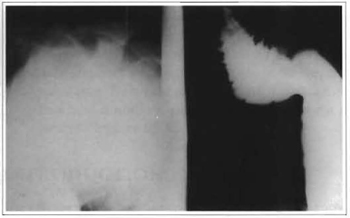
Fig. 7 -30th PO day -Microsurgical jejunal flap. No fistulas and adequate flow in the contrast X-ray.
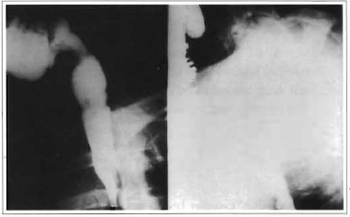
Fig. 8 -A lower view of the exam.
Despite technical progress, general survival rates still are low and the prognosis depends on staging. Most lesions are in advanced stages(2,8). The general mortality rate is 30% in 5 years and in advanced stages greater than 90%, with a survival of 20% in 1 year(8,9). Within this context, surgery aims to improve quality of life. The choice of the technique is controversial, and the indication must be adjusted to each patient. The advantages of both techniques described include the possibility of resecting and reconstructing in a single and simultaneous time, lower complication rate, shorter hospitalization period and the fact that non-irradiated tissue can be used. The indication for using these techniques in our patients was based on the features and site ofcervical defects after tumor resections. Up to now (9 month minimum follow-up) , none of the reconstructions performed presented any complications (stenosis, fistulas, infection, necrosis), thus allowing the patient to return to an oral diet, representing a significant improvement in the quality of life of these patients, with comfort and dignity.
REFERENCES
1. STELNICKI EJ, JONES TR. Surgery of the head and neck. In: DOHERTY GM, BAUMANN DS, CRESWELL LL, editors -The Washington manual of surgery. 34th ed. Little Brown, ed. 1997. p.4607.
2. CASTRO FM. Reconstrução do trânsito alimentar após faringolaringectomias. In: BRANDAO LG, FERRAZ AR, editores -Cirurgia de cabeça e pescoço. 2a ed. Ed. Roca, 1989. p.295-318.
3. JONES NF. Free jejunal transfer. In: MYERS EN, CARRAU RL, CASS SP, editors. Operative otolaryngology, head and neck surgery. WB.Saunders, ed. 1997. p.758-62.
4. SIEWERT JR, HOLSCHER AH. Jejunal interposition in esophageal replacement. In : NYHUS LM, BAKER RJ, FISHER JE, editors. Mastery of Surgery. 2nd ed. Little Brown, ed. 1992. p.802-12.
5. ANTHONY JP, SINGER MI, DESCHLER DG, et al. Long-term functional results after pharyngoesophageal reconstruction with the radial forearm free flap. Am J Sur;g. 1994; 168:4415.
6. YAMAMOTO Y, MINAKAWA H, FUKUDA S, et al. Reconstruction following total laryngopharyngoesophagectomy and extensive resection of the superior mediastinum. Plast. Recontr. Sur;g. 1997; 99:506-10.
7. ELY JE Faringostomias. In: ELY JF. Cirurgia plástica. 2nd ed. Ed. Guanabara-Koogan, 1980. p.48792.
8. BRANDAO LG, FERRAZ AR. Tumores malignos da hipofaringe. In: BRANDAO LG, FERRAZ AR, editores. Cirurgia de cabeça e pescoço. 1ªed. Ed. Roca, 1989. p.374-6.
9. BALLANGER J, COLINS SL. Neck, pharynx, oropharynx and nasopharynx, maxilla and mandible. In: BALLANGER J, SNOW JB, editors. Otorhinolaryngology, head and neck surgery. 15th ed. William & Wilkins, ed. 1996. p. 322-58.
I - Professor of the PUCRS School of Medicine. Hand Surgeon Certified by the Brazilian Medical Association and Brazilian Hand Surgery Society. Full Member of the Brazilian Reconstructive Microsurgery Society.
II - Resident Physician of Plastic Surgery of São Lucas Hospital-PUCRS.
III - Professor of Plastic Surgery at the PUCRS School of Medicine. Certified in Plastic Surgery by the Brazilian Society of Plastic Surgery.
Address for correspondence:
Jefferson Luis Braga Silva, MD
Av. Ipiranga, 6690
Hospital São Lucas da PUCRS
Centro Clinico -Sala 216
90610-000 -Porto Alegre -RS Brazil
Phone: (55 51) 315-6277
e-mail: jeffmao@zaz.com.br
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket