



Original Article - Year 2001 - Volume 16 -
Advanced Rhinomyoplasty and Ultrasound
Rinomioplastia Avançada com Ultra-sonografia
ABSTRACT
The authors include a dynamic nasal SMAS assessment in the pre-operative routine, and then include selective myoplasties in surgical planning of the nose (rhinomyoplasties). Management and 3 month to 2 year follow-up results are described for each case. The authors conclude the study by establishing the benefits for patients in procedures in the following muscles: pyramidal, transverse, nasolabial, myrtiform (tip depressor) tip and lip elevator (all elements of the nasal structure) identified through ultrasound using the needle technique.
Keywords: Nose; rhinoplasty; nasal muscle; anatomy; myoplasty; myorhinoplasty; dynamic rhinoplasty; ultrasound
RESUMO
Os autores incluem na rotina pré-operatória a avaliação dinâmica do SMAS nasal, assim como passam a incluir as mioplastias seletivas nos planejamentos cirúrgicos do nariz (rinomioplastias). São descritas as condutas caso a caso, com resultados em follow-up de 3 meses a 2 anos. Finalizam definindo os benefícios alcançados pelos pacientes com os procedimentos, nos músculos: piramidal, transverso, nasolabial, mirtiforme (depressor da ponta), elevador da ponta e do lábio (todos os que constituem a capa nasal), identificados através da ultra-sonografia, pela técnica de agulhamento.
Palavras-chave: Nariz; rinoplastia; músculo nasal; anatomia; mioplastia; miorrinoplastia; rinoplastia dinâmica; ultra-sonografia
After studying nasal anatomy in cadavers and ratifying the work of Galli(1) JJ et al., Ramos(2), JE et al., regarding the concept ofthe nasal SMAS, we observed a subtle emphasis on the importance of ala nasi and tip muscles and started to research and analyze the movements of nasal muscles to plan rhinoplasties, having obtained excellent results after associating myoplasties to conventional procedures. We noted that many patients benefited from the choice, obtaining satisfactory results with rhinomyoplasty alone. We were encouraged by studies published by Denecke(3) HJ and Gonella(4) HA,which showed that they had achieved the same results. We can currently work safely in all muscles that comprise the muscular framework (Table I & Fig. 1), by marking them by the needle technique using ultrasound (Figs. 2a-2c). We are careful not to remove muscle aponeuroses, particularly the nasal aponeurosis, so as to prevent cutaneous damage to the tip. We recommend treating nose muscles by complete rhinomyoplasty, based on the satisfactory results achieved.
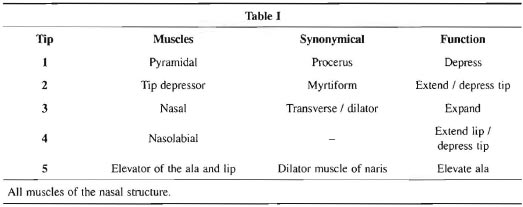
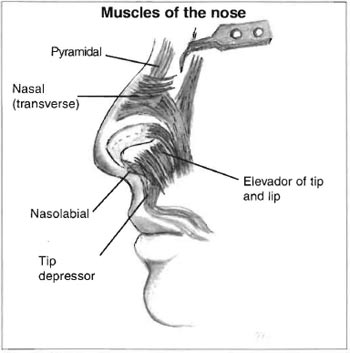
Fig. 1 -Nose anatomy.
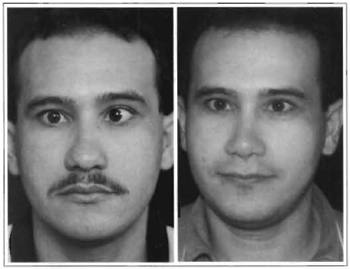
Figs. 2a & 2b - Negroid globular, wide base, wide dorsum nose. Myotonia: nasal muscle, myrtiform and wing muscle.
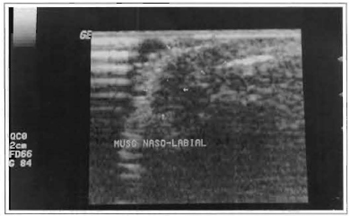
Fig. 2c - Ultrasound identifying muscles that have not been operated on.
PATIENTS AND METHODS
We studied surgical procedures and results obtained in 13 patients: 10 females and 3 males, all with dark skin and ranging in age from 17 to 56 years, who were submitted to selective nose muscle myoplasties (Figs. 3a -3c). We employed ultrasound for surgical planning (Figs. 6a-6d and 7a-7c), associated with other procedures or separately, for treating myrtiform and nasolabial muscles. All patients were submitted to local anesthesia, using a solution of 1% lidocaine with 1/100.000 epinephrine associated to sedation performed by the anesthesiologist.
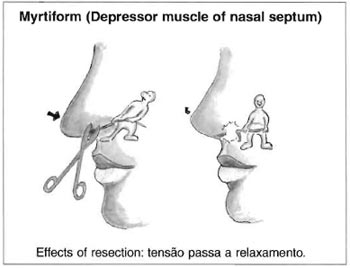
Fig. 3a -Drawing of Myotonia of the S.D.M. (Depressor muscle of nasal septum).
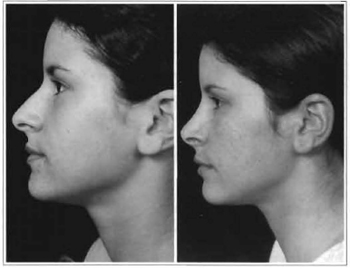
Figs. 3b & 3c -Long nose, with low hump and tip, particularly when patient smiles. Myotonia: myrtiform muscle.

Figs. 4a & 4b -Drawing of wing muscle approximation.

Figs. 4c & 4d -Negroid nose, globular tip with a broad base. Myotonia: muscles -nasal, nasolabial, tip depressor and lip elevator.

Fig. 5 -Secondary nose operated on 2 years ago. Sequela of a scar at the columella and cartilage asymmetry, globular tip. Myotonia: muscles nasolabial, myrtiform and nasal.
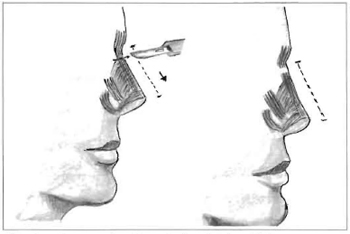
Fig. 6a -Drawing of dorsal myotonia (pyramidal).
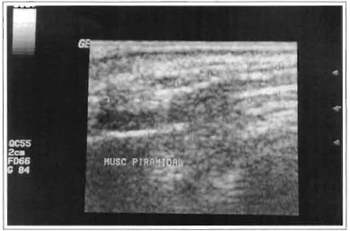
Fig. 6b -Ultrasound of precero or pyramidal muscle, identified by needle technique.

Figs. 6c & 6d -Short nose, globular tip and short columella, dorsum in sella. Myotonia: pyramidal muscle (elongation).
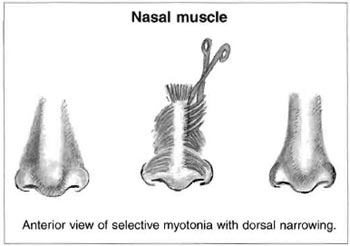
Fig. 7a -Scheme of dorsal myotonia (nasal muscle).
Figs. 7b & 7c -Long wide nose, with apparent septum deviation to the right. Low tip when patient smiles. Myotonia: nasal muscle to the right and myrtiform.
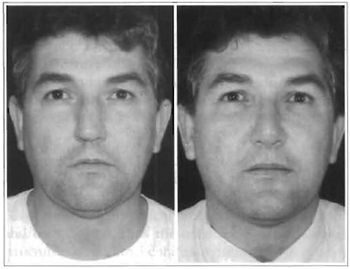
Fig. 7d -Ultrasound of transverse hypertrophic muscle to the right.
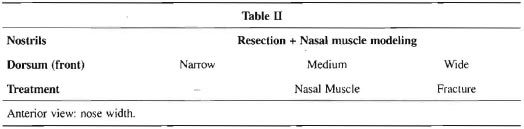
All patients were submitted to a rigorous preoperative assessment, not only for facial aesthetics but also for nasal mimics, responsible for the dynamic needed for precise rhinomyoplasties. Figures 2a-2c to 7a-7c, show mostly profile views of some of the variations performed and pre- and postoperative results, with 3 month to 2 year follow-ups. We analyzed front and profile views, particularly the positions of the lip, sella and hump (profile) and the different types of dorsum width (front), as well as the treatment of nasal framework muscles (Table II).
DISCUSSION
Although most rhinoplasty studies describe nasal SMAS in detail and some experienced authors such as Converse(5,6), Ely(7) and Pitanguy(8) have already mentioned nose movements, rhinoplasty plans did not include nasal muscles - or merely referred to their existence, at the most. More recently, other authors, have also published studies including one or two isolated muscles related to the elevation of the nasal tipobserving movement of the nari- the lifting of the tip, the opening of the nostrils and the shrinking of the nasal dorsum skin, as well as the lateral movement of the columella and the anterior portion of the cartilaginous septum. All of the studies have served as a basis for us to amplify our scope of options. In the present study, we have developed a new option to help surgeons: complete rhinomyoplasty, with positive interventions and results for all muscles of the nasal SMAS, assisted by ultrasound and by marking muscles using the Gahan and Berg(9) needle technique, and thereby facilitating and simplifying the surgical technique employed.
CONCLUSION
When we added a dynamic assessment of the nasal muscular component in our pre-operative routine for all patients with nose deformities, we pointed out the determining factor for us to refine our rhinoplasties. Myoplasties have largely benefited mestizo patients, with ala nari that open more when they smile. These patients are mostly operated on without cutaneous wing resections. The same is true for dorsal myoplasties, in which we began ro obtain a better definition in addition to better contour of the nasal tip.
Elderly patients with a lower nasal tip benefited greatly from our procedure when they were submitted to face lifts. We complemented the rhinomyoplasty with a small unilateral intra-cartilaginous opening in the nose, which allowed us ro easily reach several muscles, thus enriching facial harmony. Therefore, we recommend complete rhinomyoplasty, and the possibility of intervening in all components of the nasal SMAS by using ultrasound and marking muscles with the needle technique.
REFERENCES
1. GALLI JJL e cols. New surgical concepts -Nasal tip. Function. Anth. Plast. Surg. 1997; 21: 240242.
2. RAMOS JEA e cols. Retalho miocutaneo de músculo nasal. Rev. Soc. Cir. Plást. 1985; 0:25 32.
3. DENECKE HJ e MEYER R. Rinoplasty Plastic Surgery of. the Head and Neck. 1 Ed. New York : Springer, Verlag, 1967.
4. GONELLA HA. Contribuição ao estudo anatômico e cirúrgico dos musculos da ponta nasal. Rev. Soc. Bras. Cir. Pátist. 1998; 93:7.
5. CONVERSE JM . Reconstructive Plastic Surgery. 2 ed. Philadelphia: WB Salmders, 1977. pp. 1040-1281.
6. CONVERSE JM. Corrective Plastic Surgery of the nose. In Paparella and Shumrick, 1 Ed. Otolaringology: Head And Neck, vol. 3. Philadelphia: WB Saunders, 1973. pp. 528-599.
7. ELY JE Cirurgia Plástica. 2 ed. Rio de Janeiro : Guanabara Koogan, 1980.
8. Pitanguy I, Salgado F, Radwanski HN, Bushkin SC. The surgical importance of the dermocartilaginous ligament of the nose. Plast Reconstr Sur;g. 1995;95(5):790-4..
9. GAHAN MC, BERG G. Diagnostic Ultrasound. 1 ed. New York : Lippincott-Haven, 1998.
I - Senior member of the Brazilian Society of Plastic Surgery and ISAPS. Clinical director of Clinica Hospitalar Multiplástica.
II - Senior member of the Brazilian Society of Plastic Surgery and ISAPS.
Address for correspondence:
Moises Wolfenson, MD
Av. Joao de Barros, 791
50100-020 -Recife -PE Brazil
Phone/fax: (55 81) 3231-1621
e-mail: moiseswolfenson@hotmail.com
Work performed at Clinica de Cirurgia Plástica e Hospital Mont Sinai, Recife, Brazil
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket