



Original Article - Year 2026 - Volume 41Issue 1
Eutrophic Facelift: A Less-Invasive Alternative to Rhytidoplasty
Facelift eutrófico: alternativa menos invasiva para a ritidoplastia
Juliana Custodio Sales Di Cunto Porta1, ; Beatriz da Motta Ramos Mendonça2
; Beatriz da Motta Ramos Mendonça2
ABSTRACT
Introduction Facial aging poses significant challenges in cosmetic surgery due to anatomical, physiological, and psychological changes. Surgical techniques have evolved to address these changes while striking a balance between effectiveness and safety. Eutrophic facelift is an alternative to conventional rhytidoplasty. This less invasive technique involves minimal skin detachment and subdermal tunneling to achieve facial rejuvenation whilst preserving skin vitality.
Materials and Methods This retrospective study analyzed 53 patients who underwent eutrophic facelifts from 2017 to 2024, considering specific inclusion and exclusion criteria. The surgical technique included minimal skin undermining, subdermal tunneling with a cannula, superficial muscular aponeurotic system (SMAS) plication, and supplementary procedures as needed for each case.
Results The eutrophic facelift technique yielded satisfactory esthetic outcomes, preserving a natural and revitalized skin appearance, with minimal bruising and moderate edema, and no cases of hematoma, seroma, or necrosis. The surgical procedure reduced postoperative recovery time, resulted in hospital discharge within 24 hours, without the need for drains, and with a high satisfaction rate.
Conclusion The eutrophic facelift is a safe, less invasive, and efficient technique, with quick recovery. It also ensures natural esthetic outcomes with a low complication rate.
Keywords: rhytidoplasty; plastic surgery; minimally invasive surgical procedures; rejuvenation; skin aging
RESUMO
Introdução O envelhecimento facial é um dos maiores desafios da cirurgia estética, resultando em alterações anatômicas, fisiológicas e psicológicas. Técnicas cirúrgicas evoluíram para tratar essas mudanças, buscando equilibrar eficácia e segurança. O facelift eutrófico é apresentado como uma alternativa à ritidoplastia convencional. Essa técnica menos invasiva envolve descolamento mínimo da pele e tunelização subdérmica, visando o rejuvenescimento facial com preservação da vitalidade cutânea.
Materiais e Métodos Este estudo retrospectivo analisou 53 pacientes submetidos ao facelift eutrófico, entre 2017 e 2024, considerando critérios específicos de inclusão e exclusão. Atécnica cirúrgica incluiu descolamento mínimoda pele, tunelização subdérmica comcânula, plicatura do SMAS e procedimentos complementares, conforme necessidade de cada caso.
Resultados A técnica de facelift eutrófico apresentou resultados estéticos satisfatórios, preservando um aspecto natural e vitalizado da pele, com mínima equimose e edema moderado, sem casos de hematoma, seroma ou necrose. O procedimento cirúrgico apresentou tempo reduzido de recuperação pós-operatória e alta hospitalar em menos de 24 horas, sem uso de drenos e com alta taxa de satisfação.
Conclusão O facelift eutrófico é uma técnica segura, menos invasiva e eficaz e comrápida recuperação. Também garante resultados estéticos naturais e baixo índice de complicações.
Palavras-chave: ritidoplastia; cirurgia plástica; procedimentos cirúrgicos minimamente invasivos; rejuvenescimento; envelhecimento da pele
Introduction
Facial aging is one of the main challenges in cosmetic surgery.1 The facial contour can undergo anatomical, esthet-ic, and functional changes resulting from chronological aging and the influence of external factors, leading to physiological and psychological alterations.2 During this complex process, fat compartments change in volume, resulting in decreased thickness of the subcutaneous fat. Simultaneously, there is a reduction in muscle mass while bones lose volume and projection. These combined changes contribute to sagging of the overlying skin and the formation of wrinkles.3
Faced with the challenge of balancing intrinsic and ex-trinsic aging, plastic surgery has evolved over the centuries in the development of techniques to treat facial aging.4 Facial rejuvenation surgery has its historical roots in the 20th century. In 1901, the German surgeon Eugene von Hollander fulfilled a request from a Polish aristocratic lady by removing a wedge of skin in front of her ear to improve the sagging of her face. Although there are no detailed descriptions of the procedure, von Hollander became a pioneer of facial rhyti-dectomy.5 At the time, the procedure consisted of resections of skin wedges with approximation and suturing of the surgical edges, presenting limited outcomes.2
The 1960s represented significant technical advances in rhytidoplasty. In 1962, Gonzalez-Ulloa emphasized the im-portance of plication of the deep facial tissues, improving the outcomes.5 Since then, rhytidoplasty has undergone several evolutionary stages, including the use of associated plication and lipectomies of the lower third of the face and neck.4-6 With the advancement of scientific understanding and the consolidation of this surgery as a safe procedure, studies on the superficial musculoaponeurotic system (SMAS) highlighted the significance of treating deep facial struc-tures.2 This led to the development of techniques for SMAS treatment (dissections, concomitant traction of the skin, and liposuction replacing lipectomies), the latter being widely adopted for about 2 decades.4-6 As such, facial rejuvenation, previously a simple detachment and repositioning of cuta-neous tissue, progressed to a large mobilization of the deep facial structures.7
Literature on facelifts often reports the routine use of extensive dissections, which can result in a devitalized appearance of the skin due to damage to several nerve and vascular connections during extensive detachment. Addi-tionally, complications from rhytidoplasty have been widely discussed in the literature, encouraging many surgeons to develop techniques that reduce tissue and anatomical aggression.2
A minimal skin detachment technique can offer greater safety and better results by preserving the neurovascular trabeculae and maintaining skin vitality. In response to the growing demand for less aggressive procedures, this study aims to describe the “eutrophic” rhytidoplasty (from the Greek eu, meaning “well,” and trophein, “to nourish”), which consists of subdermal tunneling of the face and neck with the aid of a cannula, associated with conventional minimal detachment around the auricle. The proposed technique is less invasive and, at the same time, maintains the wide reach and effectiveness of regular rhytidoplasty.6
Objective
The present study aims to describe the technical details and validate the eutrophic facelift as a less invasive, safer, and more effective technique, with minimal detachment and satisfactory outcomes in facial rejuvenation.
Materials and Methods
The current retrospective, uncontrolled, interventionalclinical study analyzed a sample of 53 patients, aged between 46 and 75 years, who underwent rhytidoplasty using the eutrophic facelift technique from 2017 to 2024 at a private hospital in Rio de Janeiro, Brazil. Sociodemographic data was collected from the patients’ medical records and is detailed in ►Table 1.
| Sociodemographic data | Patients: n (%) | ||
|---|---|---|---|
| Gender | Female | 46 (82.14) | |
| Male | 7 (12.50) | ||
| Ethnicity | Caucasian | 50 (89.29) | |
| Black | 3 (5.36) | ||
| Smokers | Yes | 7 (12.50) | |
| No | 46 (82.14) | ||
| Total | 53 (100) | ||

The inclusion criteria were patients with facial aging and excess skin who underwent a eutrophic facelift technique, with one of the authors as primary surgeon in all cases during the study period. The exclusion criteria were patients who underwent rhytidoplasty using another surgical tech-nique or without the author as primary surgeon.
The combination of the presented technique with surgical procedures was considered, such as small liposuction in areas of adipose hypertrophy, blepharoplasty, resection of a small skin spindle in the submental region, lobuloplasty, lipofilling, and lip lifting, as well as nonsurgical procedures, such as ablative lasers, robotic microneedling, and hyalur-onic acid fillers. The author provided postoperative care, and all patients signed the Informed Consent Form (ICF).
Summary of the surgical steps
1. Antisepsis and bilateral marking for a eutrophic facelift.
2. Local anesthesia with sedation and infiltration with stan-dard anesthetic solution.
3. Minimal skin detachment, of approximately 3 to 4 cm, with scissors, around the auricle.
4. Subdermal tunneling performed with a cannula through-out the nondetached area and in the cervicomandibular region.
5. The SMAS plication technique was used in the direction of best traction.
6. Traction of the dermocutaneous flap upwards and backwards.
7. Flap fixation in the preauricular and retroauricular regions.
8. Resection of excess dermocutaneous flap.
9. Sutures.
Surgical technique
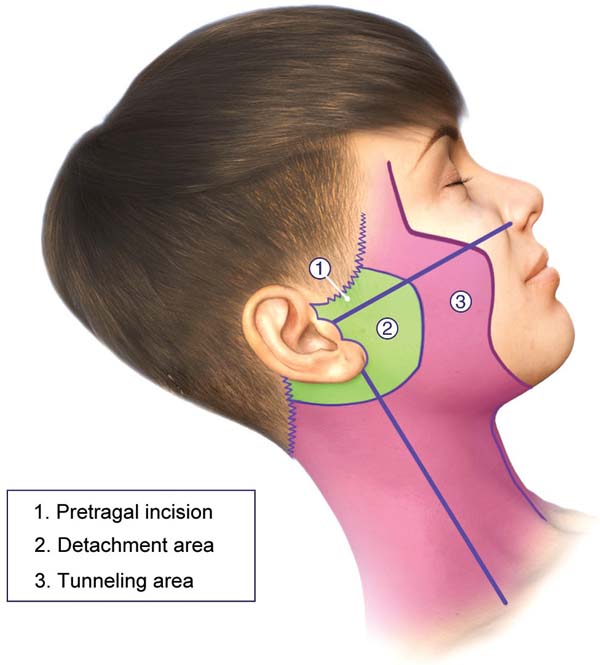
The characteristic bilateral marking for a eutrophic facelift is performed with the patient awake, seated on the edge of the bed, according to the standardization. First, marking the incision along the sideburn, descending to the preauricular region in a pretragal position, contouring the lobulus auriculae towards the retroauricular region, and following the topogra-phy of the retroauricular muscle towards the hairline. Then, marking the area for dissection within a 3 to 4 cm radius around the auricle and marking the limit of the tunneling area, approximately 1 cm from the orbital rim, descending medially towards the nasolabial fold, and ending approximately 2 cm from the labial commissure. This helped define the quadrants for systematizing the tunneling through a line that goes from the lobulus auriculae to the nasal alae, from the lobulus auriculae perpendicularly to the sternocleidomastoid, a mid-line from the chin to the sternal notch, and two lines parallel to the clavicles. ►Fig. 1 depicts the markings described here.

At this time, if applicable, the marking of lipodystrophy areas for liposuction, upper and/or lower blepharoplasty, skin flaps in the submental region to be resected, lobulo-plasty, areas for lipofilling, lip lifting, and potential areas for filling are also carried out.
All patients underwent local anesthesia with sedation. Anesthetic infiltration was performed with a 1:200 thousand adrenaline solution, consisting of 140 mL of 0.9% saline solution, 40 mL of 2% lidocaine, 20 mL of 7.5% ropivacaine, and 1 mL of adrenaline, totaling 200 mL and covering the dissection and tunneling areas.
Through a pretragal incision and a trichophytic incision in the hair implantation area, the premarked area is detached, in a radius of approximately 3 to 4 cm, around the auricle,8 in the subdermal plane, first with a scalpel, followed by scissors (►Fig. 2).


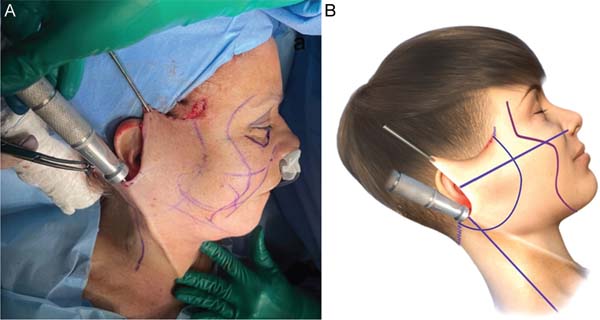
Next, the pre-marked areas on the face and cervicoman-dibular region are tunneled using 3 and 4 mm caliber lipo-suction cannulas, respectively (►Fig. 3A,B).
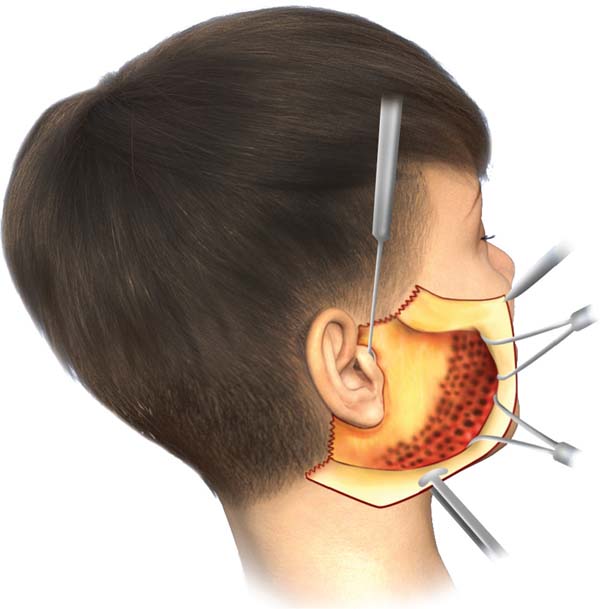
The preservation of trabeculae after subdermal tunneling shows the integrity of vascular connections (►Fig. 4) with the skin, demonstrating mobilization and traction similar to that observed in more extensive dissections (►Fig. 5).6



According to Daher and Muñiz,6 SMAS plication is per-formed with interrupted sutures using 3-0 nylon, keeping the knots inverted. The suture line follows the direction of greatest traction of deep structures. Then, traction of the excess skin is performed following the force vectors: one in a predominantly cephalic direction and another in a poster-osuperior direction, following the tragus-tubercle line of Darwin, as described by Pitanguy,9 without contradicting the direction of SMAS traction and respecting the natural tendency most suitable for each face (►Fig. 5).
The skin flap is blocked using 4-0 nylon sutures in the pre-and retroauricular regions. The excess skin is removed, adjusting to the markings, preserving the zigzag incision to maintain the trichophytic scar.
Continuous suturing uses 5-0 nylon in the anterior hair implantation areas, 6-0 nylon in the preauricular region, 5-0 nylon in the retroauricular region, and 4-0 nylon in the retroauricular hair region, with a running suture in the anterior region and a Greek bar in the retroauricular region, without the need for drains. Lastly, a compressive dressing with Zobec (Medi House) and a crepe bandage is applied, remaining in place until the patient is discharged the follow-ing day.
Results
The proposed technique yielded satisfactory esthetic out-comes, both in terms of facial rejuvenation and the preser-vation of a natural and revitalized appearance of the tissue. ►Figs. 6-11 show the results of two patients included in this study.












In the postoperative period, there was almost no bruising, and the edema was moderate, as shown in ►Figs. 12 and 13. There were no cases of hematoma, seroma, or tissue necrosis. One patient presented with neuropraxia of the marginal branch of the mandibular nerve, which completely and spontaneously resolved after 5 months.




Postoperative recovery was considerably reduced com-pared with the technique used in conventional rhytidoplas-ties, ensuring patients were in ideal condition for hospital discharge in less than 24 hours after surgery.
No patient required drains since the remaining detached area after SMAS plication was minimal. All patients who underwent eutrophic facelift in this retrospective study expressed satisfaction with the outcomes.
Discussion
The eutrophic facelift technique differs from conventional rhytidoplasty due to minimal skin detachment, focusing on subdermal tunneling. This procedure spares the neurovascular trabeculae, resulting in skin with a nourished appearance, avoiding the artificial and devitalized look that can occur with other techniques.6 Furthermore, this ap-proach ensures a more comprehensive repositioning of tissues and structures that undergo anatomical migration due to aging,10,11 as the preservation of the trabeculae allows for the traction not only of the dermocutaneous flap but also of deeper structures. In this way, the outcomes of the eutrophic facelift technique were satisfactory, natural, and safe.
The eutrophic facelift technique was first described and widely disseminated by Daher and Muñiz,6 to limit conventional skin dissection around the auricle to a 3 to 4 cm radius, reduce the detached area, minimize dead spaces, eliminate the need for drains, and ensure skin eutrophy by preserving the neurovascular trabeculae. The authors reported an approximately 50% reduction in surgical time compared to conventional rhytidoplasty due to the proce-dure’s less invasive nature.6 This study confirms the decrease in surgical time, allowing the desired effect to be achieved in a shorter recovery period and minimizing patient discomfort.12-14
The most frequent complication in facial lifting proce-dures is hematoma,15 which can occur due to minor bleeding resulting from increased blood pressure, mainly in the retroauricular region.16 However, since eutrophic facelift considerably reduces the dissected area, the incidence of hematomas is negligible in procedures that follow this technique.8,13 Additionally, the proposed technique reduces the risk of vascular and nerve injuries and eliminates the need for drains, allowing the patient to immediately return to social life after surgery, being discharged in less than 24 hours after the procedure.
The indication for the eutrophic facelift technique is broad, encompassing patients who present with signs of aging such as skin laxity, fat accumulation, SMAS ptosis, deep wrinkles, and prominent platysmal bands, without exclud-ing smokers. Smoking is a significant risk factor for skin flap impairment, since nicotine in microcirculation reduces tis-sue survival due to its thrombogenic effect.15 The proposed technique may be particularly suitable for smokers due to the preservation of trabeculae and consequent blood perfusion, which minimizes risks compared to more invasive procedures.
Supplementary surgical procedures, such as liposuction in areas of fat hypertrophy during the subdermal tunneling stage, can optimize outcomes in selected patients.17,18 Ad-ditionally, submental skin resection, blepharoplasty, lobulo-plasty, lipofilling, and lip lifting can be combined with the procedure. The association of nonsurgical procedures, such as ablative lasers, robotic microneedling, and hyaluronic acid fillers, can lead to better outcomes. All these approaches were deemed viable alternatives when conducting this study.
Conclusion
Eutrophic facelift can be considered a less invasive, safe, and effective technique, providing reduced postoperative recov-ery compared to conventional rhytidoplasty. The proposed approach presents a high success rate due to its less invasive nature and low complication rate, ensuring natural esthetic outcomes.
REFERENCES
1. Rohrich RJ, Yalamanchili H, Janis JE, Gunter JP. Rhytidoplasty fundamentals. Surg Cosmet Dermatol 2010;2(01):9-15
2. Saldanha OR, Azevedo SFD, Saldanha OR Filho, Saldanha CB, Chaves LO. Facelift with composite undermining. Rev Bras Cir Plást 2010;25(01):135-140
3. Machado BHB. Pitanguy’s Technique on Rhytidoplasty. In: Avelar JM, editor. Aesthetic Facial Surgery. Cham, Switzerland: Springer; 2021:17-31
4. Daher M. Lipofacelift: plástica facial com descolamento mínimo. Arq Catarin Med 2009;38(Suppl 1):220-223
5. Avelar JM, Martire L Junior. History of Rhytidoplasty. In: Avelar JM, editor. Aesthetic Facial Surgery. Cham, Switzerland: Springer; 2021:511-519
6. Daher M, Muñiz AR. The eutrophic rhytidoplasty: Subdermal tunneling and minimal skin undermining. Eur J Plast Surg 2013;36(02):87-94. Doi: 10.1007/s00238-012-0767-2
7. Miró AL, Fernandes JW. The Technique and Legacy of the Lateral SMASectomy to Rhytidoplasty. In: Avelar JM, editor. Aesthetic Facial Surgery. Cham, Switzerland: Springer; 2021:497-508
8. Stocchero IN. Shortscar face-lift with the RoundBlock SMAS treatment: a younger face for all. Aesthetic Plast Surg 2007;31 (03):275-278. Doi: 10.1007/s00266-006-0197-2
9. Pitanguy I. The round-lifting technique. Facial Plast Surg 2000;16(03):255-267. Doi: 10.1055/s-2000-13622
10. Graf R, Groth AK, Pace D, Graça L Neto. Facial rejuvenation with SMASectomy and FAME using vertical vectors. Aesthetic Plast Surg 2008;32(04):585-592. Doi: 10.1007/s00266-008-9173-3
11. Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg 2007; 119(07):2219-2227. Doi: 10.1097/01.prs.0000265403.66886.54
12. Ramirez OM. Full face rejuvenation in three dimensions: a “face-lifting” for the new millennium. Aesthetic Plast Surg 2001;25(03): 152-164. Doi: 10.1007/s002660010114
13. Litner JA, Adamson PA. Limited vs extended face-lift techniques: objective analysis of intraoperative results. Arch Facial Plast Surg 2006;8(03):186-190. Doi: 10.1001/archfaci.8.3.186
14. O’Connell JB. Refinements of minimal-incision rhytidectomy. Eur J Plast Surg 2003;26(06):312-318. Doi: 10.1007/s00238-003-0545-2
15. Pitanguy I, Machado BH. Facial rejuvenation surgery: a retros-pective study of 8788 cases. Aesthet Surg J 2012;32(04):393-412. Doi: 10.1177/1090820X12438895
16. Bersou A Júnior. Complications in Rhytidoplasty: How to Prevent and Treat Them. In: Avelar JM, editor. Aesthetic Facial Surgery. Cham, Switzerland: Springer; 2021:875-885
17. Teimourian B. Face and neck suction-assisted lipectomy associa-ted with rhytidectomy. Plast Reconstr Surg 1983;72(05): 627-633. Doi: 10.1097/00006534-198311000-00006
18. Daher JC, Cosac OM, Domingues S. Face-lift: the importance of redefining facial contours through facial liposuction. Ann Plast Surg 1988;21(01):1-10. Doi: 10.1097/00000637-198807000-00001
1. Departament of Plastic Surgery, Clínica Dra. Juliana Sales, Rio de Janeiro, RJ,
Brazil
2. Pharmacy School, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil
Address for correspondence Juliana Custodio Sales Di Cunto Porta, Departamento de Cirurgia Plástica, Clínica Dra. Juliana Sales, Avenida Afonso Arinos de Melo Franco 222, Bloco 1, Sala 305, Barra da Tijuca, Rio de Janeiro - RJ, CEP: 22631-455, Brazil (e-mail: julianaplastica@icloud.com).
Article received: April 14, 2025.
Article accepted: August 12, 2025.
Editor-in-Chief: Dov Charles Goldenberg.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket