



Original Article - Year 2025 - Volume 40Issue 1
Evaluation of a Surgical Tactic in the Prevention of Oronasal Fistula during Palatoplasty in Patients with Cleft Palate
Avaliação de uma tática cirúrgica na prevenção de fístula oronasal durante a palatoplastia em pacientes fissurados
Géza Lászlo Urményi1, ; Elizabeth Castineira Fernandes1; Lucas Gábor Urményi1
; Elizabeth Castineira Fernandes1; Lucas Gábor Urményi1
ABSTRACT
Oronasal fistula is a common complication in surgeries for the repair of cleft palate. It represents a challenge due to the scarcity of tissue in the affected area. The incidence of this complication ranges from 3% to 46%, and it is more prevalent in zone III of the Pittsburgh classification, which corresponds to the junction between the hard and soft palates. The present study aimed to evaluate a surgical tactic to reduce the incidence of oronasal fistulas. We conducted a retrospective study with 142 consecutive patients who underwent palatoplasty from January 2018 to June 2024 at Hospital Santa Izabel using the two-flap technique with a strategy to reduce suture tension. We analyzed factors such as cleft type (per the Veau classification), age at surgery, sex, cleft size, and fistula incidence (according to the Pittsburgh classification). The incidence of oronasal fistulas was of 1.4%, which is significantly lower than the rates reported in the literature, with no fistulas occurring in zone III, where they are more frequent. The tactic reduced fistula formation, even in patients with wide clefts and comorbidities, demonstrating its viability and benefits for the clinical practice.
Keywords: cleft palate; fistula; oral fistula; palate; hard; palate; soft
RESUMO
A fístula oronasal é uma complicação comum em cirurgias de reparo da fissura palatina, e representa um desafio devido à escassez de tecido na região afetada. A incidência dessa complicação varia de 3% a 46%, sendo mais prevalente na região III da classificação de Pittsburgh, que corresponde à junção entre os palatos duro e mole. Este estudo tem como objetivo avaliaruma tática cirúrgica para reduzir a incidência de fístulas oronasais. Realizou-se um estudo retrospectivo com 142 pacientes consecutivos submetidos à palatoplastia entre janeiro de 2018 e junho de 2024 no Hospital Santa Izabel, utilizando a técnica de 2 retalhos associada a uma tática para reduzir a tensão da sutura. Foram analisados fatores como tipo de fissura (pela classificação deVeau), idade à cirurgia, sexo, tamanho da fissura e incidência de fístulas (conforme a classificação de Pittsburgh). A incidência de fistulas oronasais foi de 1,4%, significativamente menor do que a relatada na literatura, sem ocorrência de fístulas na zona III, onde são mais frequentes. A tática mostrou-se eficaz na redução da formação de fístulas, mesmo em pacientes com fissuras amplas e comorbidades associadas, o que evidencia a sua viabilidade e os benefícios para a prática clínica.
Palavras-chave: fissura palatina; fístula; fístula bucal; palato duro; palato mole
Introduction
Oronasal fistula (ONF) is a complication that all surgeons seek to avoid due to its complexity and the need for palatal reoperation. In addition, it has implications for facial development and speech. It results from a healing failure after the first palate repair surgery, creating a patent opening between the oral and nasal cavities.
The incidence of ONF varies widely in the literature, from 3 to 46%.1–28 A recent review29 reported an incidence ranging from 6.4 to 8.6%. The Pittsburgh classification30 categorizes the ONF location into seven types: I) uvula; II) soft palate; III) soft and hard palate junction; IV) hard palate; V) primary and secondary palate junction; VI) lingual alveolar; and VII) labial alveolar. A meta-analysis6 showed an ONF incidence of 6.9% and demonstrated the occurrence of fistulas according to the Pittsburgh classification as follows: type I – 0%; type II – 15.7%; type III – 50%; and type IV – 32.6%.
Despite the several surgical techniques available for palatoplasty, the literature still lacks a consensus on the ideal approach to prevent ONF formation. A meta-analysis31 indicated the absence of a statistically significant difference between palatoplasty techniques and ONF incidence. The most common techniques present the following fistula rates: Furlow – 6.6%; double-flap – 5.1%; Wardill Kilner – 12.5%; von Langenbeck – 11.5%; Sommerland – 14.3%; and others – 6.7%.
Although many studies highlight surgeon experience as a factor associated with a lower ONF incidence, others do not find statistical significance.3,32 The cleft palate type is associated with the incidence of ONF.19 According to the Veau classification, the higher the degree, the greater the risk of developing ONF,9 with a 2.64-fold increase in the ONF index corresponding to the increase in the Veau classification. The literature is consensual25,31,33–39 on three central aspects: suture tension as the main factor for ONF formation, the relationship between the cleft width and the amount of palatal tissue available for reconstruction, and that more aggressive palatal dissections and lateral relaxing incisions can reduce suture tension, decreasing the incidence of ONF.
Objective
The current study aimed to evaluate a surgical tactic to reduce the incidence of ONF with a special focus on Pittsburgh’s zone III, which presents the highest incidence.
Materials and Methods
The Ethics Committee of Hospital Santa Izabel, in the city of Salvador, state of Bahia, Brazil, approved the present study, which was conducted at said facility. This retrospective study involved 142 consecutive patients who underwent primary palatoplasty from January 2018 to June 2024, when the new surgical tactic was introduced. We included all patients with cleft palate and lip without previous palate surgery, regardless of comorbidities or associated syndromes.
The patients were stratified according to the cleft type per the Veau classification, sex, age at surgery, and cleft width. To measure the cleft width, we used preoperative photographs and calculated the width a/b ratio, in which “a” is the cleft width and “b” is the width of the foramen of the greater palatine artery. We assessed the fistula incidence per the Pittsburgh classification. All patients were operated on by the same surgeon, using the two-flap palatoplasty technique,40 and underwent an evaluation 30 days after surgery.
The new surgical tactic was designed to reduce suture tension in Pittsburgh’s zone III, where 50% of fistulas occur. This zone is a transitional area between the hard and soft palates, with thin tissues usually sutured in two planes, one in the nasal mucosa and the other in the oral mucosa. The proposed method introduces a third suture plane in the periosteum, a tissue more resistant to traction, with one or two U-shaped Vicryl-4.0 sutures (►Figs. 1–3).
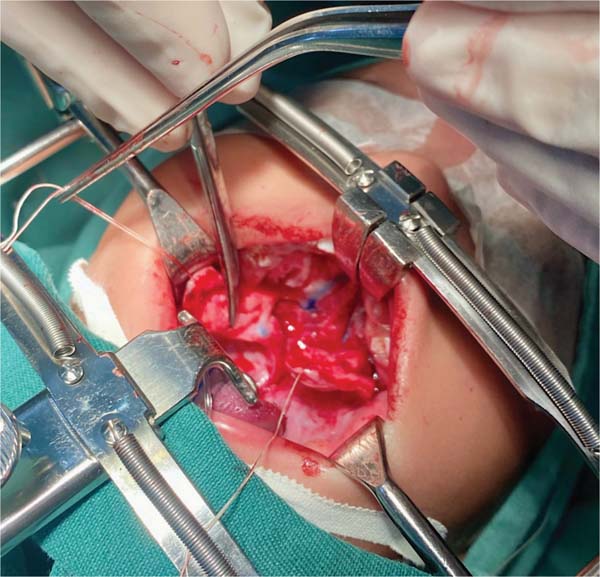

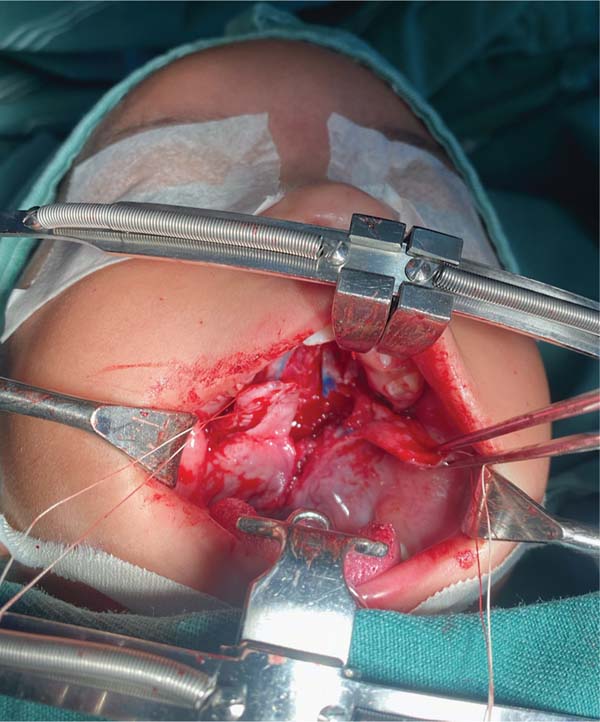



The palatoplasty was performed under general anesthesia using the two-flap mucoperiosteal technique with intravelar veloplasty, following the principles of Sommerland41 and using lateral relaxing incisions. We applied sutures to the nasal mucosa and muscles, introducing a third suture plane in the transition zone, that is, using one to two U-shaped sutures in the periosteal plane in the distal portion of the mucoperiosteal flap. Then, we closed the oral mucosa and placed hemostatic material in the bloody areas. The patients received a liquid diet for 7 days and had no hand or arm movement restrictions.
Results
The 142 patients included 59 female and 83 male subjects. According to the Veau classification, 7.04% of them were type I, 8.42% were type II, 61.26% were type III, and 23.23% were type IV. Most patients (73.23%) were younger than 24 months old at surgery, 15.49% were operated on between 24 and 47 months of age, and 11.26% were older than 48 months at surgery. The cleft width ratio was < 0.40 in 83.09% of the patients and > 0.40 in 16.09%.
| Veau classification | Sex | Age at surgery (months) | Cleft width ratio | |||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | < 24 | 24–48 | > 40 | < 40 | ≥ 40 | ||
| Type I (n) | 10 | 6 | 4 | 10 | 0 | 0 | 10 | 0 |
| Type II (n) | 12 | 7 | 5 | 6 | 5 | 1 | 9 | 3 |
| Type III (n) | 87 | 55 | 32 | 67 | 11 | 9 | 80 | 7 |
| Type IV (n) | 33 | 20 | 13 | 21 | 6 | 6 | 19 | 14 |

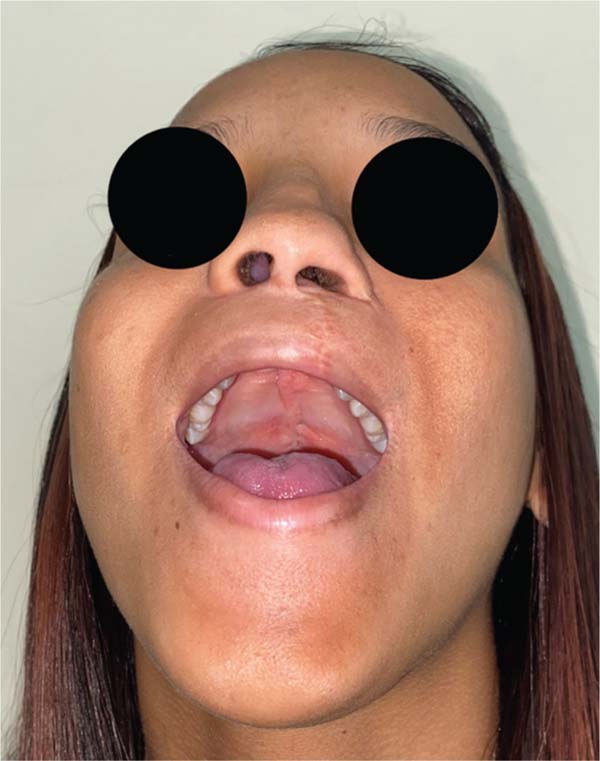
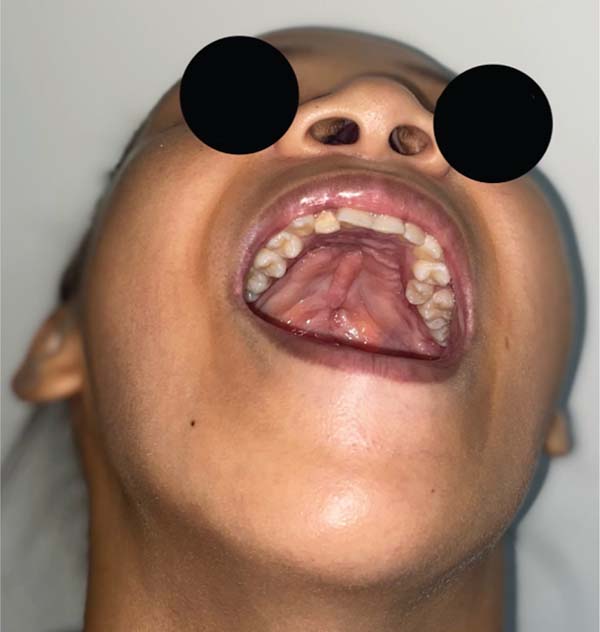
The overall incidence of ONF was of 1.4%, affecting 2 patients classified as Veau type IV, who were younger than 24 months, had a cleft width ratio > 0.40, and the fistulas were located in zone II.
Further analysis revealed that one of these patients had a behavioral disorder with repetitive hand-to-mouth movements, as reported by the mother. In the second case, preoperative photographs revealed a velopalatine fossa and inadequate dissection by the surgeon, which contributed to fistula formation (►Figs. 4–11).














Discussion
Effective ONF prevention remains a crucial goal in palatoplasty. Closure of the ONF often results in more scarring in the palate and adjacent areas, requiring additional surgical procedures. Regardless of the surgical technique for cleft palate closure, the incidence of ONF persists. Some studies suggest that surgeon experience is associated with lower ONF rates, while others find no statistical difference.
The sex and age distribution of patients undergoing surgery remains consistent with those reported in other published studies. Regarding the causes of ONF formation, the cleft type is a significant factor, with an increased risk according to the Veau classification. The cleft size and the amount of tissue available for closure are directly linked to suture tension, making them valuable predictors of ONF. Lateral relaxing incisions are essential for tension reduction. Although 16.09% of the patients in the current study presented high cleft width, introducing the third suture plane lowered ONF rates, demonstrating its effectiveness.
Pittsburgh’s zoneIII,lying at the junctionbetween the hard and soft palates, presents the highest ONF rate due to high suture tension and thin tissues. Introducing a third periosteal suture plane in Pittsburgh’s zone III was an innovative attempt to minimize the tension in the mucoperiosteal flaps, a critical factor in healing failure. Distributing the suture tension force throughout a higher amount of periosteal tissue may have contributed to the significant decrease in ONF in the present study.
In the analysis of the cases of fistula in zone II, we identified a behavioral disorder in one subject, with a diagnosis of mild autism and maternal reports of repetitive hand-to-mouth movements, and, in another subject, a velopalatine fossa in preoperative photographs, indicating inadequate dissection as the cause of the condition. It is crucial to study ONF cases individually to understand the contributing factors and optimize the surgical approach to reduce its incidence.
Conclusion
The surgical tactic introduced showed significant results in decreasing ONF incidence in patients undergoing primary palatoplasty. Although the results were encouraging, additional prospective studies are required to validate these findings. Implementing surgical strategies and determining individual factors contributing to ONF formation are essential to further improve surgical outcomes.
REFERENCES
1. Hardwicke JT, Landini G, Richard BM. Fistula incidence after primary cleft palate repair: a systematic review of the literature. Plast Reconstr Surg 2014;134(04):618e–627e. Doi: 10.1097/PRS.0000000000000548
2. Schönmeyr B, Wendby L, Campbell A. Surgical complications in 1408 primary cleft palate repairs operated at a single center in Guwahati, Assam, India. Cleft Palate Craniofac J 2016;53(03): 278–282. Doi: 10.1597/14-206
3. Al-Nawas B, Wriedt S, Reinhard J, Keilmann A, Wehrbein H, Wagner W. Influence of patient age and experience of the surgeon on early complications after surgical closure of the cleft palate–a retrospective cohort study. J Craniomaxillofac Surg 2013;41(02): 135–139. Doi: 10.1016/j.jcms.2012.06.005
4. Becker M, Hansson E. Low rate of fistula formation after Sommerlad palatoplasty with or without lateral incisions: an analysis of risk factors for formation of fistulas after palatoplasty. J Plast Reconstr Aesthet Surg 2013;66(05):697–703. Doi: 10.1016/j.bjps.2013.01.031
5. Bekerecioglu M, Isik D, Bulut O. Comparison of the rate of palatal fistulation after two-flap and four-flap palatoplasty. Scand J Plast Reconstr Surg Hand Surg 2005;39(05):287–289. Doi: 10.1080/02844310510006529
6. Bykowski MR, Naran S, Winger DG, Losee JE. The rate of oronasal fistula following primary cleft palate surgery: a meta-analysis. Cleft Palate Craniofac J 2015;52(04):e81–e87. Doi: 10.1597/14-127
7. Daniels KM, Yang Yu E, Maine RG, Heng Y, Yang L, Shi B, et al. Palatal fistula risk after primary palatoplasty: A retrospective comparison of a humanitarian organization and tertiary hospitals. Cleft Palate Craniofac J 2018;55(06):807–813. Doi: 10.1597/16-007
8. Ha S, Koh KS, Moon H, Jung S, Oh TS. Clinical outcomes of primary palatal surgery in children with nonsyndromic cleft palate with and without lip. BioMed Res Int 2015;2015:185459. Doi: 10.1155/2015/185459
9. Kahraman A, Yuce S, Kocak OF, Canbaz Y, Guner SI, Atik B, Isik D. Comparison of the fistula risk associated with rotation palatoplasty and conventional palatoplasty for cleft palate repair. J Craniofac Surg 2014;25(05):1728–1733. Doi: 10.1097/SCS.0000000000000967
10. Li F, Wang HT, Chen YY, W-L,Liu J-Y, Hao J-S, Luo D-Y. Cleft relapse and oronasal fistula after Furlow palatoplasty in infants with cleft palate: incidence and risk factors. Int J Oral Maxillofac Implants 2017;46(03):275–280. Doi: 10.1016/j.ijom.2016.09.019
11. Lin KY, Black JS, Wang JS, Kerpelman J, Ho TVT, Borowitz K. An outcome study of a 2-flap pushback palatoplasty used in the treatment of wide cleft palates. J Craniofac Surg 2015;26(03): 620–624. Doi: 10.1097/SCS.0000000000001355
12. Moar KK, Sweet C, Beale V. Fistula Rate after primary palatal repair with intravelarveloplasty: a retrospective three-year audit of six units (NorCleft) in the UK. Br J Oral Maxillofac Surg 2016;54 (06):634–637. Doi: 10.1016/j.bjoms.2016.03.021
13. Murthy AS, Parikh PM, Cristion C, Thomassen M, Venturi M, Boyajian MJ. Fistula after 2-flap palatoplasty: a 20-year review. Ann Plast Surg 2009;63(06):632–635. Doi: 10.1097/SAP.0b013e318199669b
14. Phua YS, de Chalain T. Incidence of oronasal fistulae and velo-pharyngeal insufficiency after cleft palate repair: an audit of 211 children born between 1990 and 2004. Cleft Palate Craniofac J 2008;45(02):172–178. Doi: 10.1597/06-205.1
15. Sullivan SR, Marrinan EM, LaBrie RA, Rogers GF, Mulliken JB. Palatoplasty outcomes in nonsyndromic patients with cleft palate: a 29-year assessment of one surgeon’s experience. J Craniofac Surg 2009;20(Suppl 1):612–616. Doi: 10.1097/SCS.0b013e318192801b
16. Wilhelmi BJ, Appelt EA, Hill L, Blackwell SJ. Palatal fistulas: rare with the two-flap palatoplasty repair. Plast Reconstr Surg 2001; 107(02):315–318. Doi: 10.1097/00006534-200102000-00002
17. Lu Y, Shi B, Zheng Q, Hu Q, Wang Z. Incidence of palatal fistula after palatoplasty with levator veli palatini retropositioning according to Sommerlad. Br J Oral Maxillofac Surg 2010;48(08): 637–640. Doi: 10.1016/j.bjoms.2009.10.018
18. Yuan N, Dorafshar AH, Follmar KE, Pendleton C, Ferguson K, Redett RJ III. Effects of cleft width and Veau type on incidence of palatal fistula and velopharyngeal insufficiency after cleft palate repair. Ann Plast Surg 2016;76(04):406–410. Doi: 10.1097/SAP.0000000000000407
19. Ahmed MK, Maganzini AL, Marantz PR, Rousso JJ. Risk of persistent palatal fistula in patients with cleft palate. JAMA Facial Plast Surg 2015;17(02):126–130. Doi: 10.1001/jamafacial.2014.1436
20. Lithovius RH, Ylikontiola LP, Sándor GKB. Incidence of palatal fistula formation after primary palatoplasty in northern Finland. Oral Surg Oral Med Oral Pathol Oral Radiol 2014;118(06): 632–636. Doi: 10.1016/j.oooo.2014.07.002
21. Bardach J. Late results of multidisciplinary management of uni-lateral cleft lip and palate. Plast Reconstr Surg 1986;77(04):691
22. Muzaffar AR, Byrd HS, Rohrich RJ, Johns DF, LeBlanc D, Beran SJ, et al. Incidence of cleft palate fistula: an institutional experience with two-stage palatal repair. Plast Reconstr Surg 2001;108(06): 1515–1518. Doi: 10.1097/00006534-200111000-00011
23. Stewart TL, Fisher DM, Olson JL. Modified Von Langenbeck cleft palate repair using an anterior triangular flap: decreased incidence of anterior oronasal fistulas. Cleft Palate Craniofac J 2009; 46(03):299–304. Doi: 10.1597/07-185.1
24. Mak SYA, Wong WH, Or CK, Poon AMS. Incidence and cluster occurrence of palatal fistula after furlow palatoplasty by a single surgeon. Ann Plast Surg 2006;57(01):55–59. Doi: 10.1097/01.sap.0000205176.90736.e4
25. Emory RE Jr, Clay RP, Bite U, Jackson IT. Fistula formation and repair after palatal closure: an institutional perspective. Plast Reconstr Surg 1997;99(06):1535–1538
26. Passos VdAB, Carrara CFdC, Dalben GdS, Costa B, Gomide MR. Prevalence, cause, and location of palatal fistula in operated complete unilateral cleft lip and palate: retrospective study. Cleft Palate Craniofac J 2014;51(02):158–164. Doi: 10.1597/11-190
27. Bresnick S, Walker J, Clarke-Sheehan N, Reinisch J. Increased fistula risk following palatoplasty in Treacher Collins syndrome. Cleft Palate Craniofac J 2003;40(03):280–283. Doi: 10.1597/1545-1569_2003_040_0280_ifrfpi_2.0.co_2
28. Rodrigues HLR. Incidence ofcleft palate fistula after von Langenbeck palatoplasty with extended intravelar veloplasty. Rev Bras Cir Plást 2015;30(04):597–602. Doi: 10.5935/2177-1235.2015RBCP0198
29. Buller M, Jodeh D, Qamar F, Wright JM, Halsey JN, Rottgers SA. Cleft palate fistula: A review. Eplasty 2023;23:e7
30. Smith DM, Vecchione L, Jiang S, Ford M, Deleyiannis FWB, Haralam MA, et al. The Pittsburgh Fistula Classification System: a standardized scheme for the description of palatal fistulas. Cleft Palate Craniofac J 2007;44(06):590–594. Doi: 10.1597/06-204.1
31. Landheer JA, Breugem CC, van der Molen ABM. Fistula incidence and predictors of fistula occurrence after cleft palate repair: two-stage closure versus one-stage closure. Cleft Palate Craniofac J 2010;47(06):623–630. Doi: 10.1597/09-069
32. Tse RW, Siebold B. Cleft palate repair: Description of an approach, its evolution, and analysis of postoperative fistulas. Plast Reconstr Surg 2018;141(05):1201–1214. Doi: 10.1097/PRS.0000000000004324
33. Parwaz MA, Sharma RK, Parashar A, Nanda V, Biswas G, Makkar S. Width of cleft palate and postoperative palatal fistula–do they correlate? J Plast Reconstr Aesthet Surg 2009;62(12): 1559–1563
34. Sommerlad BC. Cleft palate repair: Early anterior palatal closure and intravelar veloplasty techniques. In: Global Cleft Care in Low-Resource Settings. Springer International Publishing; 2021: 177–188
35. Mahoney MH, Swan MC, Fisher DM. Prospective analysis of presurgical risk factors for outcomes in primary palatoplasty. Plast Reconstr Surg 2013;132(01):165–171. Doi: 10.1097/PRS.0b013e3182910acb
36. Cohen SR, Kalinowski J, LaRossa D, Randall P. Cleft palate fistulas: a multivariate statistical analysis of prevalence, etiology, and surgical management. Plast Reconstr Surg 1991;87(06):1041-–1047 10.1097/00006534-199106000-00005
37. Eberlinc A, Koželj V. Incidence of residual oronasal fistulas: a 20year experience. Cleft Palate Craniofac J 2012;49(06):643–648. Doi: 10.1597/10-146
38. Amaratunga NA. Occurrence of oronasal fistulas in operated cleft palate patients. J Oral Maxillofac Surg 1988;46(10):834–838. Doi: 10.1016/0278-2391(88)90044-4
39. Chae JH, Jang HJ, Hong IP, Kim JH. A review of oronasal fistula following palatoplasty in recent 10 years. J Korean Soc Plast Reconstr Surg 1998;25(06):1003–1008
40. Bardach J. Atlas of Craniofacial and Cleft Surgery. Vol 2;Philadel-phia: Lippincott Raven; 1999
41. Sommerlad BC. A technique for cleft palate repair. Plast Reconstr Surg 2003;112(06):1542–1548. Doi: 10.1097/01.PRS.0000085599.84458.D2
1. Plastic Surgery Service, Hospital Santa Izabel, Salvador, BA, Brazil
Ethics Committee Number
Financial Support The authors declare that they did not receive financial support from agencies in the public, private, or non-profit sectors to conduct the present study.
Clinical Trials None.
Address for correspondence Géza Lászlo Urményi, Serviço de Cirurgia Plástica, Hospital Santa Izabel, Salvador, BA, Brazil (e-mail: geza701@gmail.com).
Article received: December 15, 2024.
Article accepted: February 06, 2025.
Conflict of Interests The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket