



Case Report - Year 2026 - Volume 41Issue 1
Experience with Tarsoconjunctival Flap in Eyelid Reconstruction after Tumor Resection at the Brazilian National Cancer Institute
Experiência com retalho tarsoconjuntival na reconstrução palpebral após ressecção de tumores no Instituto Nacional de Câncer
Dunia Verona1, ; Aline Mayumi Anzai1; Gabriel Neves dos Santos Mosqueira Gomes1; Jaime Enrique Durán Bustamante1; Frederico Silveira Avellar Lucas1
; Aline Mayumi Anzai1; Gabriel Neves dos Santos Mosqueira Gomes1; Jaime Enrique Durán Bustamante1; Frederico Silveira Avellar Lucas1
ABSTRACT
Eyelid reconstruction is essential for restoring function and esthetics to the periorbital region following tumor resections. The Hughes tarsoconjunctival flap is widely used for the correction of extensive lower eyelid defects, due to its good tissue integration and satisfactory outcomes. The present retrospective observational study describes 5 cases operated on at the Instituto Nacional de Câncer, Brazil, between January 2023 and May 2025.We included patients who underwent eyelid reconstruction with the Hughes flap following resection of malignant tumors, with analysis of clinical and technical data, as well as functional and aesthetic outcomes. The mean age was 71.8 years, with basal cell carcinoma being themost frequent diagnosis. All defects involved more than 50% of the lower eyelid, and the average time to flap division was 4.6 weeks. Most cases had good aesthetic and functional outcomes. One patient developed ectropion as a postoperative complication and is awaiting surgical correction. No patient presented with lesion recurrence after tumor excision. The reported experience confirms the applicability and safety of the Hughes flap as an effective option for lower eyelid reconstruction in oncologic settings. The findings are consistent with the literature and reinforce the importance of individualized planning, attention to potential complications, and careful postoperative follow-up.
Keywords: allografts; basal cell carcinoma; eyelid neoplasms; plastic surgery procedures; surgical flaps
RESUMO
A reconstrução palpebral é fundamental para restaurar a função e a estética da região periorbital após ressecções tumorais. O retalho tarsoconjuntival de Hughes é amplamente utilizado na correção de defeitos extensos da pálpebra inferior, por oferecer boa integração tecidual e resultados satisfatórios. Este estudo retrospectivo observacional descreve 5 casos operados no Instituto Nacional de Câncer, entre janeiro de 2023 e maio de 2025. Foram incluídos pacientes submetidos à reconstrução palpebral com retalho de Hughes após ressecção de tumores malignos, com análise de dados clínicos e técnicos, assim como de desfechos funcionais e estéticos. A média de idade foi de 71,8 anos, sendo o diagnóstico mais frequente de carcinoma basocelular. Todos os defeitos acometiam mais de 50% da pálpebra inferior e o tempo médio para a divisão do retalho foi de 4,6 semanas. Os resultados demonstraram boa evolução estética e funcional na maioria dos casos. Um paciente apresentou ectrópio como complicação pós-operatória e aguarda correção cirúrgica. Nenhum paciente apresentou recidiva da lesão após exérese do tumor. A experiência relatada confirma a aplicabilidade e segurança do retalho de Hughes como opção eficaz na reconstrução palpebral inferior em contexto oncológico. Os achados são consistentes com a literatura e reforçam a importância do planejamento individualizado, da atenção às possíveis complicações e do acompanhamento pós-operatório criterioso.
Palavras-chave: aloenxertos; carcinoma basocelular; neoplasias palpebrais; procedimentos de cirurgia plástica; retalhos cirúrgicos
Introduction
Eyelid reconstruction is fundamental to restoring the protective function of the eye, ensuring adequate tear film distribution, and maintaining the aesthetic harmony of the periocular region. Tumors, trauma, and previous surgeries can result in full-or partial-thickness eyelid defects, requiring surgical techniques that offer both structural stability and good functional and aesthetic outcomes.
The Hughes or tarsoconjunctival flap was introduced in 1937 by Wendell Hughes1 for the reconstruction of full-thickness eyelid defects affecting more than 50% of the eyelid. This technique has been a cornerstone of orbitopalpebral plastic surgery, due to its ability to replace tissue “on an equal footing,” using tarsoconjunctival tissue to restore both the structural and functional integrity of the eyelid. The flap consists of the tarsus of the upper eyelid. During its creation, 3 to 4 mm of tarsal height is spared at the donor site to avoid distortions of the upper eyelid margin and entropion.
The most common cause for eyelid reconstruction is the correction of defects resulting from the removal of malignant tumors, especially basal cell carcinoma (BCC), which predominantly affects the lower eyelid. Several studies consistently indicated that oncological resection is the main indication for this reconstruction. Furthermore, BCC is the most frequent histopathological subtype requiring surgical intervention and subsequent reconstruction to restore function and aesthetics.2,3
Objective
This study aims to describe five cases of eyelid reconstruction using a tarsoconjunctival flap, evaluating the functional and aesthetic outcomes after resection of malignant tumors at Instituto Nacional do Câncer (INCA), Brazil, from 2023 to 2025, and to report this institute’s experience with the technique.
Materials and Methods
This retrospective observational study, approved by the Research Ethics Committee of INCA, opinion number 7.515.014, occurred from January 2023 to May 2025. The study included all patients who underwent eyelid reconstruction using a Hughes tarsoconjunctival flap, performed by the Plastic Surgery service of INCA, after resection of malignant eyelid tumors.
The inclusion criteria were patients undergoing eyelid reconstruction with Hughes flap; with complete medical records including clinical, operative, and photographic data; and who signed the Informed Consent Form (ICF), including authorization for image use.
The exclusion criteria were cases in which the Hughes flap was initially planned but not performed; patients with a lack of adequate postoperative follow-up for evaluation of aesthetic and functional outcomes; those with incomplete medical records; and those who refused to sign the ICF.
Data analysis included: clinical and anatomopathological characteristics of the tumors, technical details of the reconstruction, postoperative complications, flap division time, and clinical follow-up. Functional evaluation considered eyelid closure, ocular lubrication, and absence of ectropion. The aesthetic evaluation relied on photographic records and subjective clinical observations by the attending surgeons.
Results
Case 1
A 68-year-old man presented with squamous BCC of the left lower eyelid (► Fig. 1). The patient underwent resection with wide margins and reconstruction with a tarsoconjunctival and infraorbital dermofat flap, followed by temporary tarsorrhaphy (► Figs. 2–3). Flap sectioning occurred after 3 weeks (► Fig. 4). Aesthetic and functional outcomes were excellent, and the patient presented no symptoms of xerophthalmia (► Fig. 5).










Case 2
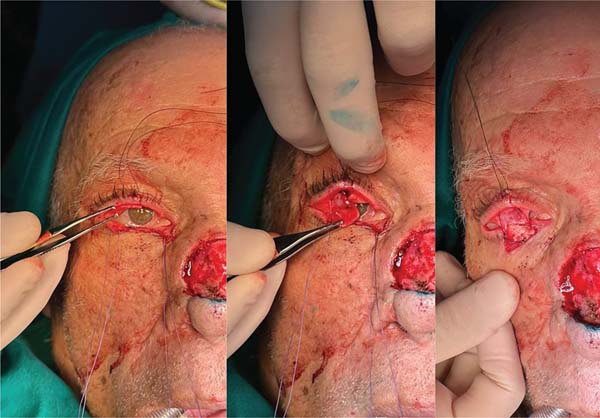
A 73-year-old man with a history of multiple BCC resections and Bowen’s disease presented with new lesions on the right lower eyelid, nasal dorsum, and malar region (► Fig. 6). The patient underwent extensive resection and reconstruction with Hughes tarsoconjunctival and advancement flaps, in addition to local grafts (► Fig. 7). However, the patient presented with new lesions on the ear, confirmed as BCC, and their treatment is under planning (► Fig. 8).





Case 3
A 78-year-old man presented with nodular BCC of the left lower eyelid. The patient underwent a wide resection and reconstruction using a tarsoconjunctival flap, which was sectioned after 3 weeks. He developed mild nocturnal lagophthalmos without local recurrence. However, a new lesion appeared on the nasal ala, confirmed as ulcerated BCC. The patient is waiting for a new surgery (► Fig. 9).


Case 4
A 73-year-old man presented with BCC of the right lower eyelid (► Fig. 10). Wide resection resulted in a 15 mm defect, reconstructed with a tarsoconjunctival flap (► Fig. 11). Flap sectioning occurred after 9 weeks. The patient had a satisfactory aesthetic outcome with no signs of recurrence (► Fig. 12).






Case 5
A 67-year-old man, with a history of melanoma on his back (2021), presented with a tumor on his left lower eyelid and a lesion on his right ear (► Fig. 13). He underwent wide resection and reconstruction with a tarsoconjunctival flap (eyelid) and local graft (ear), as shown in ► Fig. 14. Histopathology revealed infiltrative BCC in both lesions, with free margins. Flap sectioning occurred after 3 weeks. The patient developed ectropion in the medial portion of the left lower eyelid (► Fig. 15).






This study evaluated five patients who underwent reconstruction using a Hughes flap over 2 years (► Table 1). Their mean age was 71.8 years, and the primary etiology was BCC. The average time for Hughes flap section was 4.6 weeks, and the defect size was greater than 50% of the eyelid in all cases.
| Case report | Age | Histopathological diagnosis | Location | Surgical defect | Reconstruction | Time until flap sectioning | Follow-up |
|---|---|---|---|---|---|---|---|
| 1 | 68 | Squamous/infiltrative BCC | Left lower lid | > 50% of the eyelid, full thickness | Tarsoconjunctival flap+infraorbital dermofat flap | 3 weeks | Excellent aesthetic/functional outcome, with no xerophthalmia |
| 2 | 73 | Moderately differentiated BCC | Right lower eyelid | > 50% eyelid | Tarsoconjunctival flap+advancement flap | 5 weeks | Good eyelid closure and satisfactory aesthetics |
| 3 | 78 | Nodular BCC (eyelid) | Left lower eyelid | > 50% eyelid | Tarsoconjunctival flap+retroauricular graft | 3 weeks | Satisfactory aesthetics; mild lagophthalmos; new nasal lesion under surgical planning |
| 4 | 73 | BCC (eyelid) + papilloma (internal canthus) | Right lower eyelid | > 50% eyelid (15 mm) | Tarsoconjunctival flap | 9 weeks | Satisfactory aesthetics, no local recurrence |
| 5 | 67 | Infiltrative BCC (eyelid and ear) | Left lower eyelid + right ear | > 50% eyelid + ear | Tarsoconjunctival flap+local graft | 3 weeks | Development of medial ectropion in the left lower eyelid |
Abbreviation: BCC, basal cell carcinoma.

The minimum postoperative follow-up was 6 months. All patients had a satisfactory evolution in terms of periorbital functionality and aesthetic, except for one, who presented with ectropion in the late postoperative period and is scheduled for surgical correction. This patient had a history of smoking and altered blood sugar levels. On the 1st postoperative day, he presented with an area of congestion in the lateral third of the skin advancement flap, which contributed to poor healing and outcome.
There were two patients who presented with recurrence of tumor lesions in an area other than that of the eyelid resection and are currently undergoing surgical planning for removal, with subsequent reconstruction.
The patients were instructed on postoperative care, which included the use of eye drops containing an antibiotic agent and corticosteroids for 5 to 7 days, artificial tears or sodium carmellose eye drops every 4 hours in both eyes, and lubricating gel at night.
Discussion
Nonmelanoma skin cancer is the most frequent type of cancer in Brazil, accounting for approximately 30% of all malignant tumors registered in the country.4 The current main indication for eyelid reconstruction is the resection of malignant tumors, with BCC being the most common, representing about 80 to 90% cases in this region.5,6
Eyelid reconstruction is a complex surgical approach due to several interrelated factors. The eyelid is a highly specialized structure with intricate anatomy, composed of multiple tissue layers (skin, muscle, tarsus, and conjunctiva), each with distinct aesthetic and functional roles.7 Reconstruction requires precise reconstitution of the anterior and posterior lamellae to preserve eyelid mobility, protect the ocular surface, and achieve a satisfactory aesthetic outcome.8 Even small defects can compromise the delicate balance necessary for eyelid closure, tear film distribution, and corneal protection, leading to complications such as ectropion, ptosis, lagophthalmos, or exposure keratopathy if not meticulously managed.9
The surgical challenge is further increased by the need to match the color, texture, and thickness of the tissues, as well as to preserve or reconstruct the eyelid margin and canthal tendons, structures essential for both function and appearance. The proximity to the eyeball and lacrimal apparatus increases the risk of ocular injury, demanding careful intraoperative technique. Furthermore, the choice of reconstructive method must be individualized, considering the size of the defect, its location, and the involvement of adjacent structures, often requiring a combination of local flaps, grafts, or regional flaps, each with its own technical particularities and potential complications.10
There are two main reconstructive options for full-thickness defects of the lower eyelid: the Hughes flap, which uses tissue from the upper eyelid to reconstruct the posterior lamella, requiring an advancement flap or skin graft for the anterior lamella; and the Mustardé flap, which, in contrast, provides coverage for the anterior lamella of the lower eyelid, requiring a graft for the posterior lamella.11
Eyelid reconstruction with the Hughes flap occurs in two surgical stages. In the first stage, the tarsoconjunctival flap is advanced to fill the defect in the posterior lamella of the lower eyelid. Next, this flap can be covered by a full-thickness skin graft or different skin flaps, such as a malar advancement in patients with laxity, to replace the corresponding anterior lamella.
The first stage of the Hughes procedure results in a conjunctival bridge (the flap pedicle) extending from the upper eyelid across the visual axis, remaining in place for approximately 4 to 6 weeks. In the second stage, this vascularized conjunctival bridge undergoes sectioning. Although the blood supply to the reconstructed lower eyelid may be adequate after 2 weeks, the likelihood of ectropion development is greater if the separation occurs before the usual 4 to 6-week interval.8 The eyelid-sharing technique provides superior aesthetic and functional outcomes, resulting in a dynamic, mobile lower eyelid. Its main disadvantage is the need for two surgical stages.11
The Mustardé flap offers the advantage of allowing com-plete reconstruction of the lower eyelid in a single surgical procedure, making it more suitable for deep vertical defects, especially when the vertical dimension is larger than the horizontal dimension. Limitations of this technique include extensive facial scarring and the nondynamic nature of the reconstructed lower eyelid.
Technically, the flap is designed in a semicircular shape, starting at the lateral canthus of the eye and extending to the preauricular region. The flap’s superior border projects near the eyebrow level to ensure an adequate amount of tissue, and achieving a proper height helps to counterbalance the retraction of the lower eyelid margin. Elevation can be performed in the subcutaneous plane or in the sub-superficial musculoaponeurotic system (SMAS) plane, increasing blood supply. Auricular cartilage can provide posterior la-mellar lining and support. After flap rotation, medial fixation is made to the posterior branch of the medial canthal tendon or to the periosteum of the medial orbital margin. The lateral canthus is reconstructed by fixation to the inner surface of the lateral orbital margin.12
The ultimate goal of any eyelid reconstruction is to achieve an aesthetically ideal restoration of anatomy and function with minimal surgical morbidity. Carefully reconstructing the bilamellar eyelid structure is critical. The surgeon must create an anterior lamella with adequate and aesthetically appropriate skin, preserving the dynamic function of the orbicularis oculi muscle whenever possible, and form a posterior lamella that replaces the tarsus at the eyelid margin, ensuring a smooth mucosal surface that protects and preserves the cornea.10
The case studies presented in this study are consistent with the literature, reinforcing the use of the tarsoconjunctival flap as a safe and effective reconstructive technique for extensive lower eyelid defects, resulting in satisfactory aesthetic and functional outcomes.13–15
This study has limitations inherent to its retrospective nature and the small number of cases. Another relevant aspect is the lack of standardized and objective tools to measure aesthetic and functional outcomes, such as systematized photographic records, validated scales, or quality-oflife questionnaires specific to eyelid reconstruction, as suggested by previous studies.16,17 Future prospective studies with larger samples may contribute to the consolidation of these findings, as well as allow for a more robust comparative evaluation between different reconstructive techniques.
Conclusion
The present study, through INCA’s experience with the Hughes tarsoconjunctival flap for lower eyelid reconstruction after oncological resections, confirmed the applicability and safety of this established technique. The five cases evaluated had satisfactory aesthetic and functional outcomes, with good flap integration, preservation of eyelid function, and a low incidence of complications. Despite requiring two surgical procedures, the approach proved to be a reliable and high-performance option, especially when well-indicated and carefully planned.
REFERENCES
1. Hughes WL. A NEW METHOD FOR REBUILDING A LOWER LID: REPORT OF A CASE. Arch Ophthalmol 1937;17(06):1008–1017. Doi: 10.1001/archopht.1937.00850060064005
2. Archibald LK, Gupta R, Shahwan KT, et al. Periorbital reconstruc-tive techniques following Mohs micrographic surgery or excisions: a systematic review. Arch Dermatol Res 2023;315(07): 1853–1861. Doi: 10.1007/s00403-022-02523-z
3. Savur F. Surgical Reconstruction in Malignant Eyelid Tumors. J Craniofac Surg 2025;36(01):282–285. Doi: 10.1097/SCS.0000000000010703
4. Ministério da Saúde. Instituto Nacional de CâncerEstimativa 2023: Incidência de Câncer no Brasil [Internet]. Rio de Janeiro: Instituto Nacional de Câncer, 2022:162. Available from: https://www.inca.gov.br/sites/ufu.sti.inca.local/files/media/document/estimativa-2023.pdf
5. Baş Z, Sharpe J, Yaghy A, Zhang Q, Shields CL, Hyman LIRIS Registry Analytic Center Consortium. Prevalence of and Associated Factors for Eyelid Cancer in the American Academy of Ophthalmology Intelligent Research in Sight Registry. Ophthalmol Sci 2022;3(01): 100227. Doi: 10.1016/j.xops.2022.100227
6. Hirt B, Worma MB, Ogata FE, Bortolotto AP, Rastelli GJC, Kormann RB. Eyelid tumors: epidemiological profile and clinical diagnostic hypothesis accuracy. Rev Bras Oftalmol 2022;81:e0023. Doi: 10.37039/1982.8551.20220023
7. Li E, Chambers CB. Diseases of the Eyelids and Orbit. Med Clin North Am 2021;105(03):551–562. Doi: 10.1016/j.mcna.2021.02.007
8. Chang EI, Esmaeli B, Butler CE. Eyelid Reconstruction. Plast Reconstr Surg 2017;140(05):724e–735e. Doi: 10.1097/PRS.0000000000003820
9. Orgun D, Hayashi A, Yoshizawa H, et al. Oncoplastic Lower Eyelid Reconstruction Analysis. J Craniofac Surg 2019;30(08):2396-–2400. Doi: 10.1097/SCS.0000000000005639
10. Holds JB. Lower Eyelid Reconstruction. Facial Plast Surg Clin North Am 2016;24(02):183–191. Doi: 10.1016/j.fsc.2016.01.001
11. Codner MA, McCord CDJ. Eyelid and Periorbital Surgery. 2a ed. Boca Raton: CRC Press; 2016:1248
12. Codner MA, McCord CD, Mejia JD, Lalonde D. Upper and lower eyelid reconstruction. Plast Reconstr Surg 2010;126(05):231e-–245e. Doi: 10.1097/PRS.0b013e3181eff70e
13. Borges K, Chedid R, Dibe M, Sbalchiero J, Leal P. Reconstrução de pálpebra inferior com retalho modificado de Hughes: análise de resultados e complicações no Instituto Nacional de Câncer Rio de Janeiro, Brasil. Rev Bras Cir Plást 2010;25(3, Suppl 1):23
14. Souza C, Souza M, Souza R, Neves C. Reconstrução palpebral inferior em oncologia com técnica de Hughes: análise de 11 casos. Rev Bras Cir Plást 2012;27(03, Suppl 1):38
15. Golcman R, Golcman B, Pinto DS, Freitas Rda SReconstrução de pálpebra inferior pela técnica de Hughes. Arq Bras Oftalmol 1995; 58(01):42–46. Doi: 10.5935/0004-2749.19950090
16. Klassen AF, Cano SJ, Grotting JC, et al. FACE-Q Eye Module for Measuring Patient-Reported Outcomes Following Cosmetic Eye Treatments. JAMA Facial Plast Surg 2017;19(01):7–14. Doi: 10.1001/jamafacial.2016.1018
17. Ramanathan D, Chu S, Prendes M, Carroll BT. Validated Outcome Measures and Postsurgical Scar Assessment Instruments in Eyelid Surgery: A Systematic Review. Dermatol Surg 2021;47(07): 914–920. Doi: 10.1097/DSS.0000000000003077
1. Plastic Surgery Division, Instituto Nacional de Câncer, Rio de Janeiro, RJ, Brasil
Data Availability
Clinical Trials None.
Financial Support The authors declare that they did not receive financial support from agencies in the public, private or nonprofit sectors to conduct the present study.
Address for correspondence Dunia Verona, MD, MHSE, Instituto Nacional de Câncer, Cirurgia Plástica, Rio de Janeiro, RJ, BraZil (e-mail: veronadunia@gmail.com; duniaverona@hotmail.com).
Article received: March 28, 2025.
Article accepted: October 13, 2025.
Conflict of Interests The authors have no conflict of interests to declare.
Editor-in-Chief: Dov Charles Goldenberg.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket