



Review Article - Year 2026 - Volume 41Issue 1
Indications and Outcomes of the Clinical and Surgical Treatments of Lipedema: A Literature Review
Indicações e resultados dos tratamentos clínico e cirúrgico do lipedema: uma revisão bibliográfica
Amanda Rocha Meira de Melo Soares1 ; Bruno Gildo Dalla Vecchia Morales1; Jéssica Mara Bergonzini da Silva1; Sophia Sandes Siqueira Barros1,; Sthephane Georgia Honorato de Azevedo1
; Bruno Gildo Dalla Vecchia Morales1; Jéssica Mara Bergonzini da Silva1; Sophia Sandes Siqueira Barros1,; Sthephane Georgia Honorato de Azevedo1
ABSTRACT
Introduction Lipedema is a chronic disease characterized by symmetrical and painful accumulation of subcutaneous fat, influenced by genetic and hormonal factors, and frequently misdiagnosed as obesity or lymphedema.
Materials and Methods In the present narrative review, we searched the PubMed and SciELO databases for articles published between 2015 and 2025, in Portuguese and English, addressing the diagnosis and the clinical or surgical management of lipedema.
Results In the PubMed search, we identified 299 studies, which were reduced to 106 after the removal of duplicates, with a progressive increase in publications since 2020; in the search on SciELO, we only retrieved 7 studies, all of which were also indexed in PubMed. The results reinforce that lipedema presents a complex pathophysiology, involving adipocyte hypertrophy and hyperplasia, chronic inflammation,microvascular dysfunction, and estrogen-related influence. International consensus indicates that diagnosis is essentially clinical, and that conservative treatment should be prioritized, including weight management, nutritional guidance, low-impact exercise, compression therapies, and psychosocial support. Surgical intervention, particularly tumescent or water-assisted liposuction techniques, is reserved for refractory cases and does not constitute a definitive cure. The growing alignment among consensus statements published over the past 5 years highlights the need for standardized diagnostic criteria and therapeutic protocols.
Conclusion The effective management of lipedema requires a multidisciplinary approach, continuous professional education, and strengthening of research that enable the establishment of evidence-based clinical guidelines.
Keywords: diagnosis; lipedema; literature review; surgery; treatment
RESUMO
Introdução O lipedema é uma doença crônica caracterizada por acúmulo simétrico e doloroso de gordura subcutânea, influenciada por fatores genéticos e hormonais, frequentemente confundida com obesidade ou linfedema.
Materiais e Métodos Neste estudo, realizamos uma revisão narrativa por meio de buscas nas bases PubMed e SciELO, incluindo artigos publicados entre 2015 e 2025, em português e inglês, que abordassem o diagnóstico e o manejo clínico ou cirúrgico do lipedema.
Resultados Foram identificados 299 estudos na PubMed, reduzidos a 106 após a remoção de duplicatas, com aumento progressivo de publicações após 2020; na busca na SciELO, foram recuperados somente 7 estudos já encontrados na PubMed. Os resultados reforçam que o lipedema tem fisiopatologia complexa, que envolve hipertrofia e hiperplasia adipocitária, inflamação crônica, disfunção microvascular e influência estrogênica. Há consenso internacional de que o diagnóstico é essencialmente clínico, e de que o tratamento conservador deve ser priorizado, incluindo controle ponderal, orientação nutricional, exercícios de baixo impacto, terapias de compressão e apoio psicossocial. A intervenção cirúrgica, especialmente por técnicas de lipoaspiração tumescente ou assistida por água, é reservada a casos refratários, e não representa cura definitiva. Observa-se alinhamento crescente entre consensos publicados nos últimos 5 anos quanto à necessidade de padronização diagnóstica e terapêutica.
Conclusão Por fim, o manejo adequado do lipedema depende de abordagem multidisciplinar, educação profissional contínua e fortalecimento de pesquisas que permitam consolidar protocolos baseados em evidências.
Palavras-chave: diagnóstico; lipedema; revisão de literatura; cirurgia; tratamento
Introduction
Lipedema is a chronic disease characterized by the symmetrical and disproportionate accumulation of subcutaneous fat, mainly in the lower limbs of women, sparing the hands and feet. It presents with pain and edema, has a psychological impact, and affects approximately 10% of the female population. Lipedema presents a genetic component, possibly autosomal dominant with incomplete penetrance, and is frequently associated with hormonal phases such as puberty, pregnancy, and menopause. Its pathophysiology involves adipocyte hypertrophy and hyperplasia, microvascular dysfunction, tissue hypoxia, chronic inflammation, extracellular matrix (ECM) remodeling, and fibrosis, leading to lymphatic and vascular changes. Its diagnosis is complex and commonly confused with obesity, even though lipedema is resistant to weight loss and has distinct clinical characteristics. Lipedema is classified into five types based on the distribution of body fat.1
The Brazilian Consensus on Lipedema2 and international guidelines converge in indicating non-invasive treatment as the first line of therapy, prioritizing conservative clinical management based on weight control, a balanced diet, and low-impact exercises, in particular aerobic and strength training, to improve lipid metabolism, mitochondrial function, and lymphatic drainage, in addition to reducing inflammation and oxidative stress. Treatment should be multidisciplinary, encompassing nutritional, physiotherapeutic, endocrinological, and psychological support, with a focus on adherence, self-management, and the patient’s quality of life.
Since lipedema is often underdiagnosed or confused with obesity and lymphedema due to a lack of knowledge, diagnostic consensus, and insufficient understanding of its biochemical mechanisms, a deeper comprehension of the disease is essential to improve its diagnosis and management, aiming for a better quality of life for affected subjects.
Objective
The present study aims to describe the current understanding of the pathophysiology of lipedema and its classifications, to clarify the systemic inflammatory effects caused in the pathological progression of lipedema, and to characterize the key methods employed in the clinical and, especially, surgical management of lipedema.
Materials and Methods
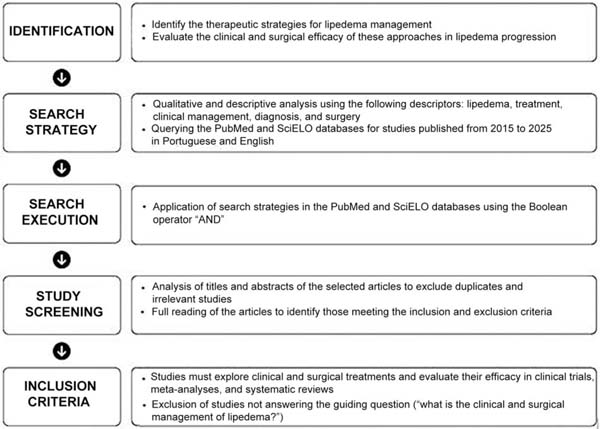
The current study consists of a qualitative and descriptive narrative review based on bibliographic research on the PubMed and SciELO databases using the descriptors lipedema, treatment, clinical management, diagnosis, and surgery, along with their Portuguese translations, applying the Boolean operator “AND” between lipedema and the remaining descriptors.
The filtering of search results respected the inclusion criteria of period, consisting of articles published between 2015 and 2025; language criteria, analyzing publications in Portuguese or English alone; publication category criteria, including clinical trials, systematic reviews, and meta-analyses; and articles that answered the guiding question (“what is the clinical and surgical managements of lipedema?”). Articles not meeting these inclusion criteria were excluded. ►Fig. 1 presents a flowchart of the steps for article inclusion.

Pathophysiology of Lipedema
Lipedema (International Classification of Diseases, 11th revi-sion [ICD-11], code: EF02.2)3 can be described as a chronic condition characterized by a disproportionate accumulation of subcutaneous adipose tissue that primarily affects the lower limbs of women, sparing hands and feet. Lipedema creates an imbalance between the upper and lower body, causes pain and edema in the affected area, and leads to psychological distress due to ongoing bodily changes.4,5 The number of underdiagnosed or misdiagnosed patients is high, despite the 10% prevalence in the general female population. Although the concept was developed 8 decades ago, its pathophysiology remains unclear, and its differential diagnosis is difficult.1
Lipedema is characterized by its progressive, disproportionate, and symmetrical expansion (mainly in the lower limbs) and fat concentration within adipocytes (hypertrophy), leading to the recruitment of immune cells and a rearrangement of the ECM. As these two events trigger inflammation and disrupt vascular and lymphatic functions, there is an accumulation of interstitial fluid, expanding the interstitial space.6
This condition has been observed in familial clusters, with 60% of patients having a first-degree relative affected by lipedema. Therefore, an autosomal dominant inheritance pattern with incomplete penetrance is presumed in cases of genetic predisposition. Lipedema often first appears during periods of hormonal change, and it may be mediated by estrogen. The onset of the disease frequently occurs during phases such as puberty, pregnancy, and menopause.6 Furthermore, it is noteworthy that the absence of estrogen receptors results in the accumulation of subcutaneous adipose tissue, which is observed in patients with lipedema.7
One of the pathophysiological hypotheses for this condition involves primary microvascular dysfunction in the lymphatic and blood capillaries, which can be explained by an exacerbation of fat that generates a hypoxic impulse, leading to endothelial deficiency and, consequently, the expansion of angiogenesis.6
The sequence of events characterizing the lipedema phenotype involves the increased expression of genes related to mitotic clonal expansion and cell proliferation, resulting in hyperplasia. Although the increased fat content in adipocytes leading to hypertrophy has been observed in lipedema, there is controversy regarding the identification of markers associated with this event. Furthermore, adipocyte growth decreases oxygen supply and causes ECM remodeling, which involves increased sodium levels, collagen deposition, and changes to the glycocalyx, causing microangiopathy and fibrosis.5
Lipedema diagnosis remains a challenge and can lead to misdiagnosis of obesity. It is worth noting that both diagnoses can coexist; however, the clinical presentation of these diseases is quite distinct. Lipedema, for instance, presents with resistance to weight loss through severe diets or high-intensity physical activity, in contrast to obesity. Furthermore, its pathophysiology is not fully understood, with several hypotheses proposed for it.7
The clinical manifestations of lipedema consist of increased volume in the lower limbs, although it can also affect the upper limbs. The distribution of adipose tissue is disproportionate throughout the body, concentrating in the buttocks, thighs, and calves, sparing the feet and hands. Lipedema is categorized into five types based on the distribution of fat in the body. The first type is described as increased fat accumulation in the thighs, hips, and buttocks. The second type involves the knees, presenting with a cushion of fat in the inner area. The third type corresponds to fat reaching the ankles. The fourth type involves the upper limbs, and the fifth type affects only the lower part of the legs.8
Clinical Treatment of Lipedema
The Brazilian Consensus on Lipedema2 advocates prioritizing non-invasive treatment as the initial and essential approach to control the condition. Conservative clinical management must precede surgical treatment, and it plays a role in subsequent follow-up. Conservative treatment mainly focuses on alleviating symptoms, enhancing quality of life, and slowing disease progression. Multidisciplinary and systemic management measures2 include weight control with balanced nutrition and low-impact exercise, which have been described to alleviate pain and sensitivity. Compression therapies and physiotherapeutic approaches, such as complex decongestive physical therapy (CDPT), are also used to reduce edema and discomfort.
As obesity is directly related to the progression of inflammatory symptoms in lipedema, instruments to assess the risks associated with the amount of body fat are required, such as anthropometric measurements, waist-to-hip ratio, and not just body mass index (BMI).2 The German S2k guideline9 emphasizes the importance of educating patients about the negative influence of concomitant obesity and the relevance of an active lifestyle and a healthy diet. Weight reduction, in cases of overweight or obesity, can decrease limb volume.
Food and Nutrition
Nutritional guidance should prioritize lasting changes in eating habits and avoid restrictive short-term diets. The adoption of a diet that helps prevent spikes in blood glucose and insulin is recommended, as elevated insulin levels can promote fat storage and inflammatory processes. Two promising dietary approaches are the Mediterranean diet, known for its anti-inflammatory properties, and the ketogenic diet, which has shown positive effects on weight loss, inflammation, and symptoms of lipedema in various studies.9
In a single case report on ketogenic diet as a nutritional intervention for lipedema, Cannataro et al.10 stated that its key beneficial mechanisms in this condition are its anti-inflammatory action due to the control of glycemic peaks, and its regulatory capacity in managing free radicals (oxidative stress). Thus, ketogenic diet may be a useful tool in lipedema management, with results showing improvement in pain and quality of life, potentially confirming the anti-inflammatory effect of the diet. It should be noted, however, that this was a single case report, and that this diet should not be proposed as the only therapeutic option, but rather as part of a set of interventions.
Physical Exercise
The incorporation of supervised physical activities is essential in the therapeutic approach to lipedema, aiming to optimize cardiovascular health, promote mobility, and prevent secondary complications such as lymphedema.2 According to the Consensus Statement of the Italian Society of Motor and Sports Sciences,7 physical exercise induces physiological responses that act directly on the central, metabolic, and inflammatory mechanisms of lipedema; moreover, the contraction of skeletal muscles during movement acts as a pump, boosting lymphatic flow and assisting in the drainage of excess interstitial fluid, contributing to the reduction of edema, one of the main symptoms.
In the metabolic context, endurance training has proven to be an effective modulator of mitochondrial function in adipose tissue. This optimization contributes to improved lipid metabolism, counteracting abnormal patterns of fat storage. In the inflammatory axis, physical activity exerts a significant impact by suppressing the chronic proinflammatory microenvironment. This process occurs partially by modulating the local immune response, inhibiting the infiltration of M1 macrophages and stimulating their phenotypic transition to M2 (anti-inflammatory) macrophages, which is associated with increased catecholamine secretion.7
Additionally, physical training promotes beneficial structural adaptations in the adipose tissue itself. One of the key mechanisms is the browning of white adipose tissue to beige fat. This phenomenon is mediated by myokines, such as irisin, whose release by skeletal muscle is dependent on the activation of peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α). It also improves tissue health by promoting angiogenesis, resulting in greater per-fusion and oxygenation, which can mitigate the hypoxic conditions frequently observed in advanced stages of lipedema. Moreover, exercise strengthens the tissue’s antioxidant defenses, improving the cells’ ability to withstand oxidative stress.7
To ensure adherence and safety for patients with lipedema, low-impact activities that minimize joint stress should be prioritized. Aquatic exercises, such as swimming and water aerobics, are highly recommended, as the hydrostatic pressure of the water acts as natural compression, helping to reduce edema, and buoyancy decreases the impact on the joints. Strength training, also known as weightlifting, plays a crucial role in managing lipedema. In addition to strengthening, increased muscle mass raises resting metabolism, helping to control body weight.7
However, the prescription must be individualized according to the patient’s pain symptoms and mobility. To achieve the best therapeutic outcomes while minimizing risks, the program should be designed by a qualified physical education professional knowledgeable about lipedema, who can tailor activities to fit the individual limitations of each patient.2 Strength training should incorporate gradual load progression and emphasize correct movement execution to prevent injuries. Pain monitoring is a fundamental aspect. Exercise should not cause significant pain, and any excessive discomfort should be a signal to adjust the program.7
Low-impact aerobic exercises, such as walking, cycling, and elliptical training, are excellent to improve cardiovascular capacity and endurance without overloading the joints. Practicing activities that promote flexibility and mobility, such as stretching and yoga, is also beneficial, as it helps relieve stiffness and improve range of motion. Wearing compression garments, such as socks or bandages, during exercise can enhance the benefits by improving tissue support, optimizing lymphatic flow, and reducing swelling.7
Furthermore, in addition to the physical benefits, the impact of exercise on the mental health and quality of life of patients with lipedema is invaluable. Living with a chronic, painful disease that affects body image can lead to anxiety and depression. Physical exercise is a key mood regulator, promoting the release of endorphins and improving the perception of well-being. Improved functional capacity and autonomy also contribute to increased self-esteem and overall quality of life.7
Compression Therapies
One of the cornerstones of the conservative lipedema treatment, according to the S2k guideline,9 is CDPT, whose main goal is not the reduction of adipose tissue, but rather the relief of pain and other subjective symptoms, such as the sensation of heaviness and tension in the affected limbs. External compression helps reduce interstitial edema, improves venous and lymphatic return, and provides tissue support, resulting in a significant decrease in discomfort. The guideline emphasizes that the choice of material and compression level requires a high level of tailoring according to the patient’s anatomy, the severity of symptoms, and their ability to adhere to treatment.9
The use of devices, such as elastic stockings, offers additional control over symptoms. However, the progression of the condition can bring challenges, such as discomfort and difficulty adapting the devices to limb disproportion.2 Therefore, in addition to customizing compression garments, the use of the lowest level of compression that provides adequate symptomatic relief to optimize adherence is recommended. For limbs with wide variations in circumference or tissue folds, flat-knitted fabric is preferable due to its greater rigidity, which prevents the formation of constrictions.9
Medical Treatment
The multidisciplinary team has several medical and health specialties, each with a specific function. The vascular surgeon, for instance, can manage associated lymphatic complications. Endocrinology care focuses on the patient’s metabolic and hormonal profiles, and gynecologists also play a relevant role in managing hormonal issues. Orthopedists may be consulted about musculoskeletal conditions caused by excess weight in the limbs. It is essential to highlight the importance of an accurate professional diagnosis to prevent ineffective treatments that could heighten patient frustration.2
According to the American consensus statement,11 medi-cal treatment of lipedema is not based on medications that cure the condition, but rather on a pharmacological and supplemental approach focused on mitigating symptoms and managing comorbidities. The main guideline is to avoid drugs that may exacerbate the condition, such as those that promote weight gain or increased edema. Diuretics, for instance, should be avoided for chronic use, as they do not address the inflammatory cause of edema in lipedema. Similarly, thiazolidinediones are contraindicated because they increase subcutaneous adipose tissue.
Conversely, sympathomimetic amines can be considered for the treatment of edema, and metformin is an option for patients with metabolic complications due to its potential to inhibit tissue fibrosis.11 The use of beta-adrenergic agonists, flavonoids, and selenium has been suggested, but their actual effectiveness in lipedema still needs elucidation and scientific confirmation.12
Psychosocial Therapy and Self-Management
The psychosocial impact of lipedema is significant, and the German guideline9 recommends the inclusion of psychosocial factors in the diagnostic assessment. Psychological disorders, such as depression and eating disorders, can affect symptoms and quality of life, and their treatment must be a priority. Psychological support, provided by psychiatrists or other mental health professionals, is considered essential to address the emotional and psychological aspects, which are often neglected.2
Enhancing patient self-management is a crucial part of their treatment. Patients should be encouraged to take an active role in their care, developing, together with the healthcare team, strategies for problem-solving and realistic therapeutic goals. Success in self-management increases self-efficacy and can lead to relevant long-term clinical improvements.9
Indications and Approaches to the Surgical Treatment of Lipedema
Regarding surgical management, Brazil was one of the pioneers in recognizing and developing a technique that avoids visible scars and enables the complete resection of the deforming tissue through a single skin flap. The approach involves making an extensive downward incision that follows the gluteal sulcus. This incision is directed forward around the deformity and pulled upward until it reaches the posterior iliac spine. Theoretically, this technique facilitates the repair of the irregularity and provides some correction of the laxity in the inner thigh.13
However, advances in medical research have shown controversies regarding the applicability of surgical procedures. There is a general agreement that surgical intervention should not occur before conservative clinical treatment, which should constitute the initial and fundamental step in managing the disease, maintaining its importance even when surgical intervention is subsequently necessary.2
Conservative management of lipedema has widely recognized benefits and should be prioritized over any invasive intervention. It is recommended to adopt and comprehensively evaluate conservative therapies for at least 1 year before considering surgical procedures.2 The therapeutic choice should result from a careful and joint analysis between the clinician, the surgeon, and the patient, based on the understanding that the main goal is functional recovery, especially regarding mobility, followed by symptom alleviation. In more advanced stages of the disease, in which there is significant locomotor disability, surgical intervention may be indicated earlier.14
The main surgical intervention for lipedema is liposuction. The main surgical techniques include tumescent liposuction (TL) and water-assisted liposuction (WAL). For TL, the tumescent solution is infused into the subcutaneous tissue to increase adipocyte volume and contract blood vessels, followed by fat aspiration with blunt-tipped microcannulas. For WAL, a pressurized jet of tumescent fluid detaches fat cells from the connective tissue, eliminating the need for conventional cannulas. Unlike traditional liposuction, TL and WAL use local anesthetics present in the tumescent solution, eliminating the need for general anesthesia.14
Data from the United States11 has revealed that women with lipedema who underwent surgery noted a decrease in affected tissue, including a reduction in disease stage and pain, as well as improvements in energy levels, strength, and walking ability. The results were reported by women at various stages of lipedema, including those with lymphedema. However, the number of reports of abnormal adipose tissue growth after surgery, within the treatment area or not, was significant. Abdominal fat redistribution was demonstrated by dual X-ray absorptiometry scans performed after thigh-suction lipectomy in patients who presented with disproportionate accumulation of adipose tissue in the lower abdomen, hips, or thighs. This finding leads us to conclude that, while surgical intervention may offer initial benefits, it does not provide a definitive cure for lipedema. Therefore, continuing conservative therapy after surgery is essential to achieve lasting results and enhance the quality of life for patients.
Results and Discussion
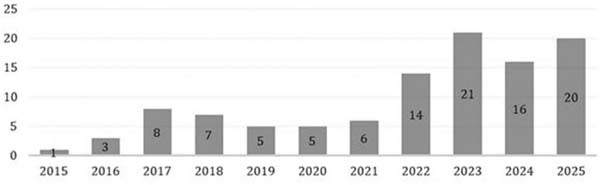
In the PubMed search, we found 299 studies published from 2015 to 2025 (►Table 1). After excluding duplicates, 106 studies remained. Considering unique results from the searches alone, the year 2023 had the highest number of publications, with 21 studies. The year 2025, although not yet concluded by the time of writing this paper, had a total of 20 published works, the second highest to date.
| Descriptor | Total | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 | 2025 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment | 105 | 4 | 5 | 8 | 12 | 5 | 7 | 6 | 11 | 18 | 13 | 16 |
| Clinical management | 53 | 3 | 3 | 4 | 3 | 3 | 4 | 4 | 4 | 8 | 9 | 8 |
| Diagnosis | 82 | 2 | 4 | 7 | 8 | 5 | 4 | 7 | 8 | 14 | 10 | 13 |
| Surgery | 59 | 2 | 2 | 6 | 5 | 2 | 2 | 3 | 9 | 13 | 10 | 5 |
| Total | 299 | 11 | 14 | 25 | 28 | 15 | 17 | 20 | 32 | 53 | 42 | 42 |

Despite the drop in 2024 compared to 2023 and considering that 2025 was not yet concluded at the time of writing, there is a notable increase in the number of studies published throughout the selected period, especially from 2022 onwards (►Fig. 2).

In the SciELO search, we found no results for all the descriptors and inclusion criteria. Therefore, we decided to search only for the descriptor lipedema, which resulted in only 7 studies: 2 from 2020, 1 from 2022, 2 from 2024, and 2 from 2025. Comparing the search results from PubMed and SciELO, all studies found by SciELO were also found on PubMed, indicating that the SciELO database was not relevant regarding the topic of lipedema.
Lipedema represents a significant contemporary medical challenge due to the complexity of its pathophysiology, widespread underreporting of cases, and its potential to generate negative biopsychosocial impacts on patients. Because of the difficulty in accurately diagnosing lipedema, which is often confused with obesity or lymphedema, the prevalence of this disease may be underestimated, contributing to inadequate therapeutic approaches.15 Recognizing lipedema as an autonomous clinical condition rather than a mere esthetic issue is essential to manage patients holistically with evidence-based interventions focused on quality of life.
Lipedema is rare in men, predominantly affecting postpubertal and adult women, who start to present symptoms between puberty and the third decade of life.5 In global estimations, lipedema affects 11% of these women, with an estimated incidence of 1 in 9 women in the United States.5,11 In Europe, a German study reported a 39% prevalence rate among 62 women.16 The only study to date that outlines the epidemiological profile of lipedema in Brazil is by Amato et al.,1 who used a software to develop a mathematical formula based on the projection of the 2021 Brazilian population census to determine diagnostic specificity at 77.8%; this study, which observed only women aged 18 to 69, estimated that 8.8 million of these subjects have symptoms suggestive of a lipedema diagnosis, representing 12.3% of the Brazilian female population.
Knowledge of several aspects of lipedema pathogenesis is still evolving in scientific studies, and the presence of family history in approximately 60% of the cases suggests the existence of a genetic component linked to the X chromosome, either autosomal or dominant. Williams syndrome, resulting from a microdeletion of approximately 1.6 million base pairs in chromosome 7q11.23, which includes the elastin precursor gene (ELN), also results in lipedema of genetic etiology.15
Moreover, as the condition tends to manifest during puberty, pregnancy, and menopause, a potential hormonal influence is implied,17 since estrogen is associated with the distribution of adipose tissue in women, mainly in the gluteal and femoral region.
Studies5 have shown increased expression of the aromatase gene (CYP19A1) in patients with lipedema, leading to a greater conversion of androgenic hormones into estrogen, but with no alteration in the levels of estrogen receptors. Protein expression and cytobiological studies15 of lipoaspi-rates from patients with lipedema suggest that these changes primarily occur in the early stages of cell differentiation during adipogenesis. The expansion of adipose tissue leads to a proinflammatory hormonal pattern and tissue hypoxia since blood vessels cannot keep up with the rapid growth of adipose tissue. This results in high expression of proinflammatory factors, such as hypoxia-inducible factor-1-alpha (HIF1α), which induce inflammation in adipose tissue.18 Such interaction involving genetic and endocrine factors creates a metabolic environment favorable to adipocyte hypertrophy and hyperplasia, triggering a cascade of inflammatory and structural events in adipose tissue.
In addition to classification by different types,8 lipedema can also be categorized into stages that differ in their progression if left uncontrolled, or regression, if properly managed (►Table 2). These 3 stages5 are the following: stage 1 features smooth skin and circumscribed, bilateral fat accumulation in the extremities; in stage 2, the skin presents an uneven or corrugated appearance with more prominent adipose tissue deposits; and stage 3 presents with a marked increase in the size of the extremities, disfiguring fat deposits that project in large masses, thickening of the subcutaneous layer with macronodular changes, and extensive sclerosis and fibrosis. An additional stage, 4, is characterized by the association with lymphedema, resulting in lipolymphedema.5
| Stages | Hallmark finding |
|---|---|
| Stage 1 | Smooth and soft skin surface with increased underlying hypodermis |
| Stage 2 | Irregular skin with pearl-sized palpable nodules (peau d’orange) |
| Stage 3 | Large fat deposits, especially on the thighs and around the knees |
| Stage 4 | Association with lymphedema |

The studies analyzed in the current research also aimed to establish a consensus on lipedema, addressing its pathophysiological definition, accurate diagnosis, differential diagnosis, and the clinical and surgical managements. Over the past 5 years, there have been 6 attempts to reach a consensus on the disease, published in various countries, which reflect their unique realities. This highlights the ongoing relevance of the topic. ►Table 3 presents the points of greatest agreement among the studies for the established consensuses.
| Consensus axis | Relevant details |
|---|---|
| Disease definition | Lipedema is a chronic condition, distinct from obesity and lymphedema, characterized by a disproportionate, painful accumulation of subcutaneous fat |
| Diagnosis | Essentially based on clinical criteria, excluding other causes and supported by imaging (ultrasound and magnetic resonance imaging) when necessary |
| Main symptoms | Pain, tenderness, bruising, a feeling of heaviness in the lower limbs, edema that worsens throughout the day |
| Staging | Classification into stages (1–3) and anatomical types (1–5) |
| Multidisciplinary approach | Management by a team including doctors, nurses, physiotherapists, nutritionists, psychologists, and physical education professionals |
| Conservative treatment | Decongestive physiotherapy, compression, nutritional control, and regular low-impact and aerobic exercise |
| Surgery | Liposuction is indicated when conservative treatment fails |
| Psychosocial support | Pain management and body image acceptance |
| Education and awareness | Reduce underdiagnosis and clinical stigma |
| Research and standardization | Need for uniform diagnostic criteria and outcomes in new studies |

In 2020, Sandhofer et al.19 proposed a consensus based on European guidelines and literature focusing on the long-term benefits of surgical treatment using TL. In the same year, Bertsch et al.18 published another attempt at a European consensus, suggesting what they call “paradigm shifts” related to lipedema, mainly regarding its clinical aspects. In 2021, the American consensus was established using the Delphi methodology, led by Herbst et al.11 These authors developed 85 statements regarding the pathophysiology and treatment recommendations for lipedema, along with suggestions for future research topics. In 2024, two consensus statements were published. The first, by theGermanSociety of Phlebology andLymphology,9 is a guideline with 60 recommendations aimed at optimizing the diagnosis and treatment of lipedema. The second one, by the Italian Society of Motor and Sports Sciences and the Italian Society of Phlebology,7 focused on establishing the importance of physical exercise as a non-pharmacological therapeutic approach to lipedema. The most recent published consensus is Brazilian, from authors representing the Brazilian Society of Angiology and Vascular Surgery,2 who applied the Delphi method to establish statements in accordance with the understanding of most researchers in the country.
From these efforts to establish a universal understanding of lipedema, the impetus of societies and organizations in multiple countries to determine the knowledge that will serve as a foundation to address this disease is noteworthy. This movement has been ongoing for the last 5 years, recognizing that, despite lipedema being a unique disorder for decades, unifying knowledge and standardizing its approach are necessary to improve its therapeutic methods.
Conclusion
Our findings indicate that lipedema is a chronic condition that remains underdiagnosed. The recognition of its importance in the literature has progressively increased between 2015 and 2025. Additionally, the understanding of its pathophysiology, as well as advancements in diagnosis and management, witnessed significant progress from 2020 onwards, largely due to the publication of several international consensus statements. Despite methodological differences among them, there is broad agreement that lipedema constitutes a distinct clinical entity, characterized by structural alterations of adipose tissue, chronic inflammation, and hormonal influence, requiring an eminently clinical diagnosis and a multidisciplinary approach. There is also consensus that conservative treatment should be the first-line therapy for lipedema, with emphasis on weight control, targeted exercise, compression therapies, and psychosocial support, reserving surgical interventions for re-fractory and severe cases as a complement to clinical measures.
The consensus statements herein analyzed further reinforce the urgent need for global standardization of diagnostic criteria and therapeutic outcomes, given the current heterogeneity of the literature. Thus, it becomes evident that progress in lipedema care depends on consolidating these efforts, continuously training healthcare professionals, and strengthening research that enables the establishment of more consistent, effective, and reproducible protocols for the appropriate treatment of the disease.
REFERENCES
1. Amato ACM, Amato FCM, Amato JLS, Benitti DA. Prevalência e fatores de risco para lipedema no Brasil. J Vasc Bras 2022;21: e20210198. Doi: 10.1590/1677-5449.202101981
2. Amato ACM, Peclat APRM, Kikuchi R, et al. Consenso Brasileiro de Lipedema pela metodologia Delphi. J Vasc Bras 2025;24: e20230183. Doi: 10.1590/1677-5449.202301831
3. Organização Mundial da Saúde (OMS) Classificação Estatística Internacional de Doenças e Problemas Relacionados à Saúde: Décima Primeira Revisão (CID-11). Genebra: OMS; 2024
4. Brenner E, Forner-Cordero I, Faerber G, Rapprich S, Cornely M. Body mass index vs. waist-to-height-ratio in patients with lipo-hyperplasia dolorosa (vulgo lipedema). J Dtsch Dermatol Ges 2023;21(10):1179–1185. Doi: 10.1111/ddg.15182
5. Poojari A, Dev K, Rabiee A. Lipedema: Insights into Morphology, Pathophysiology, and Challenges. Biomedicines 2022;10(12): 3081. Doi: 10.3390/biomedicines10123081
6. Kruppa P, Georgiou I, Biermann N, Prantl L, Klein-Weigel P, Ghods M. Lipedema-Pathogenesis, Diagnosis, and Treatment Options. Dtsch Arztebl Int 2020;117(22-23):396–403. Doi: 10.3238/arz-tebl.2020.0396
7. Annunziata G, Paoli A, Manzi V, et al. The Role of Physical Exercise as a Therapeutic Tool to Improve Lipedema: A Consensus Statement from the Italian Society of Motor and Sports Sciences (Società Italiana di Scienze Motorie e Sportive, SISMeS) and the Italian Society of Phlebology (Società Italiana di Flebologia, SIF). Curr Obes Rep 2024;13(04):667–679. Doi: 10.1007/s13679-02400579-8
8. Mortada H, Alaqil S, Jabbar IA, et al. Safety and Effectiveness of Liposuction Modalities in Managing Lipedema: Systematic Review and Meta-analysis. Arch Plast Surg 2024;51(05): 510–526. Doi: 10.1055/a-2334-9260
9. Faerber G, Cornely M, Daubert C, et al. S2k guideline lipedema. J Dtsch Dermatol Ges 2024;22(09):1303–1315. Doi: 10.1111/ddg.15513
10. Cannataro R, Michelini S, RicolfiL, et al. Management of Lipedema with Ketogenic Diet: 22-Month Follow-Up. Life (Basel) 2021;11 (12):1402. Doi: 10.3390/life11121402
11. Herbst KL, Kahn LA, Iker E, et al. Standard of care for lipedema in the United States. Phlebology 2021;36(10):779–796. Doi: 10.1177/02683555211015887
12. Buso G, Depairon M, Tomson D, Raffoul W, Vettor R, Mazzolai L. Lipedema: A Call to Action!. Obesity (Silver Spring) 2019;27(10): 1567–1576. Doi: 10.1002/oby.22597
13. Pitanguy I. Trochanteric Lipodystrophy. Plast Reconstr Surg 1964; 34:280–286. Doi: 10.1097/00006534-196409000-00010
14. Peprah K, MacDougall D. Liposuction for the Treatment of Lipe-dema: A Review of Clinical Effectiveness and Guidelines. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545818/
15. Vyas A, Adnan G. Lipedema. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.-gov/books/NBK573066/
16. Herbst KL. Subcutaneous Adipose Tissue Diseases: Dercum Disease, Lipedema, Familial Multiple Lipomatosis, and Madelung Disease. In: Feingold KR, Ahmed SF, Anawalt B, et al., editors. Endotext. South Dartmouth, MA: MDText.com, Inc.; 2000. Available from: https://www.ncbi.nlm.nih.gov/books/NBK552156/
17. Rapprich S, Baum S, Kaak I, Kottmann T, Podda M. Treatment of lipoedema using liposuction: Results of our own surveys. Phlebologie 2015;44(03):121–132. Doi: 10.12687/phleb2265-3-2015
18. Bertsch T, Erbacher G, Elwell R. Lipoedema: a paradigm shift and consensus. J Wound Care 2020;29(Sup11b):1–51. Doi: 10.12968/jowc.2020.29.Sup11b.1
19. Sandhofer M, Hanke CW, Habbema L, et al. Prevention of Progression of Lipedema With Liposuction Using Tumescent Local Anesthesia: Results of an International Consensus Conference. Dermatol Surg 2020;46(02):220–228. Doi: 10.1097/DSS.0000000000002019
1. School of Medicine, Centro Universitário São Lucas Afya, Porto Velho, RO, Brazil
Data Availability
Financial Support The authors declare that they did not receive financial support from agencies in the public, private or non-profit sectors to conduct the present study.
Address for correspondence Sophia Sandes Siqueira Barros, FaculdadedeMedicina, Centro UniversitárioSão LucasAfya, Rua Alexandre Guimarães 1.927, Porto Velho, RO, 76804–373, Brasil. (e-mail: sophia.barrosssb@gmail.com).
Article received: November 27, 2025.
Article accepted: December 16, 2025.
Conflict of Interests The authors have no conflict of interests to declare.
Editor-in-Chief: Dov Charles Goldenberg.
Study conducted at the School of Medicine, Centro Universitário São Lucas Afya, Porto Velho, RO, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket