



Case Report - Year 2026 - Volume 41Issue 1
The Sternalis Muscle: Managing a Rare Anatomical Variant Encountered during Augmentation Mastopexy - A Case Report
O músculo esternal: manejo de variante anatômica rara encontrada durante mastopexia de aumento - Relato de caso

ABSTRACT
The sternalis muscle is a rare anatomical variant on the anterior thoracic wall, overlying the pectoralis major, with an incidence of 4 to 8%. Typically asymptomatic, it can complicate thoracic or breast surgeries, requiring adjustments in technique. The present case report describes its identification duringmastopexy with implants in a 42-year-old patient. The sternalis muscle, a vascularized structure approximately 8 cm long, was noted while elevating the pectoralis major. The surgical approach was adapted to preserve the muscle, ensuring no complications or disruptions to the operative goals. The patient recovered uneventfully, with excellent outcomes. Recognition of the sternalis muscle is critical for surgeons performing breast and thoracic procedures. Its identification and preservation in the case herein reported underscore the need for anatomical awareness to optimize outcomes. Further research is needed to understand its clinical relevance in reconstructive and esthetic surgery.
Keywords: sternalis muscle; anatomical variant; breast surgery; mastopexy with implant; dual-plane technique; anatomical variation; imaging differential diagnosis
RESUMO
O músculo esternal é uma variante anatômica rara na parede torácica anterior, sobrejacente ao músculo peitoral maior, observado em 4 a 8% dos pacientes. Embora tipicamente assintomático, pode complicar cirurgias torácicas ou mamárias, o que pode exigir ajustes técnicos. Este relato de caso descreve a identificação do músculo esternal durante uma mastopexia com implantes em uma paciente de 42 anos. Este músculo, uma estrutura vascularizada com cerca de 8 cm de comprimento, foi observado durante a elevação do músculo peitoral maior. A abordagem cirúrgica foi adaptada para preservar o músculo, assegurando a ausência de complicações ou perda dos objetivos do procedimento. A paciente se recuperou sem intercorrências, com desfechos excelentes. O reconhecimento do músculo esternal é fundamental para cirurgiões que realizam procedimentos mamários e torácicos. Neste caso, sua identificação e preservação ressaltam a necessidade de conhecimento anatômico para a otimização dos desfechos. Mais estudos são necessários para entender sua relevância clínica na cirurgia reconstrutiva e estética.
Palavras-chave: músculo esternal; variante anatômica; cirurgia mamária; mastopexia com implante; técnica dual plane; variação anatômica; diagnóstico diferencial por imagem
Introduction
The sternalis muscle is a rare anatomical variant that lies superficially along the anterior thoracic wall, parallel to the sternum and superficial to the pectoralis major.1 First described in the eighteenth century, its presence has fascinated anatomists and clinicians alike due to its rarity and variability. Found in approximately 4 to 8% of individuals, the muscle is often asymptomatic and discovered incidentally during imaging, cadaveric dissections, or surgical procedures.2
Embryologically, the sternalis muscle is believed to originate as a variation of the pectoralis major or rectus abdominis musculature, although its exact development remains debated.3 Its morphology varies significantly, ranging from a thin, tendinous structure to a fully developed muscle, and it may present unilaterally or bilaterally. Its function is unclear, as it does not seem to play a significant role in chest wall movement.
The clinical relevance of the sternalis muscle lies in its potential to mimic pathological findings on imaging, such as soft-tissue masses, and its unexpected appearance during thoracic or breast surgeries. In imaging, the muscle has been mistaken for malignancies or other abnormalities, highlighting the importance of awareness among radiologists.4 In surgery, it can present challenges during procedures such as mastectomy, implant placement, or flap-based breast reconstruction, requiring adaptations in technique to preserve its integrity and avoid complications.
The current case report describes the incidental identification of the sternalis muscle during a mastopexy with prosthesis. The discovery enabled a careful evaluation of its morphology, anatomical relationships, and implications for the surgical procedure. By reviewing the literature and presenting this case, we aim to underscore the importance of recognizing this rare variant and its potential impact on surgical and clinical outcomes.
Case
A 42-year-old woman presented for mastopexy with prosthesis to address significant breast ptosis following pregnancy and breast feeding. The patient had no history of thoracic surgery, trauma, or anatomical anomalies noted on physical examination. Preoperative imaging, including mammography, showed no abnormalities.
Intraoperative Findings
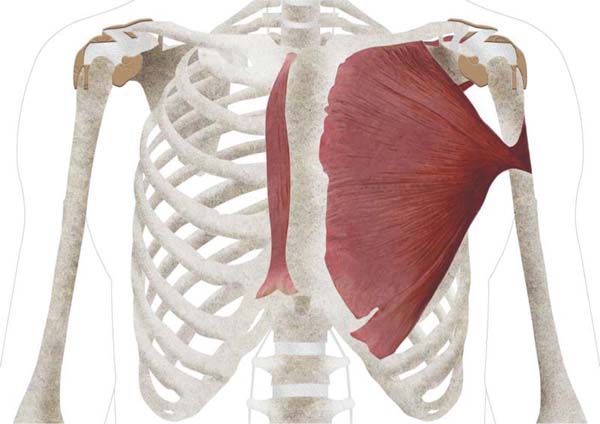
During the procedure, while elevating the pectoralis major muscle to create a dual-plane pocket for the implant, an unusual muscular structure was encountered. The muscle, located superficially to the pectoralis major and running parallel to the sternum, was identified as the sternalis muscle. An anatomical drawing of the muscle is provided in ► Fig. 1. An intraoperative video (►Vídeo 1) and picture (►Fig. 2) are also provided.



Video 1 Intraoperative video. Online content including video sequences viewable at: https://www.thieme-connect.com/products/ejournals/html/10.1055/s-0046-1818593.
The pectoralis muscle was shorter in width and did not reach the sternum. It also appeared thinner than the contra-lateral one. The sternalis muscle measured approximately 8 cm in length and 4 cm in width, had a vertical orientation, and was well vascularized. Its fibers extended from the upper thoracic region downward, following the anterior thoracic wall. The structure was distinct from both the pectoralis major and rectus abdominis, confirming its identity as a sternalis muscle.
Surgical Management
The muscle was carefully submitted to horizontal dissection to create a dual-plane pocket (created mainly by the pectoralis muscle and partly by the sternalis muscle itself). The procedure was completed without further complications, and the integrity of the muscle was maintained.
Postoperative Course
The patient experienced an uneventful recovery, with no complications related to the presence of the sternalis muscle or the surgical adjustments made. At follow-up visits, she reported high satisfaction with the esthetic results of the augmentation mastopexy. The patient achieved a BREAST-Q score of 91, indicating an excellent outcome.
Discussion
The sternalis muscle, while rare, represents a fascinating anatomical variant with significant clinical implications, particularly in thoracic and breast surgeries. Its identification during a mastopexy with implants highlights the importance of anatomical awareness in the surgical practice, as well as the need to adapt surgical techniques when confronted with such anomalies.
Anatomical and Clinical Significance
The sternalis muscle, with a reported incidence ranging from 4 to 8%, is often asymptomatic and overlooked. Its variable morphology, ranging from tendinous bands to a well-defined muscle, and unilateral or bilateral presentation make it a unique challenge for surgeons. Some researchers estimate that up to one-third of reported sternalis cases exhibit bilateral muscle fibers, while others suggest a prevalence as low as 1.7%.5 Embryologically, it is believed to arise as an aberrant development of the pectoralis major or rectus abdominis musculature. Functionally insignificant, its main relevance lies in its potential to complicate surgical procedures and imaging interpretation.6
In breast and thoracic surgeries, the muscle may pose technical challenges, such as altering the dissection plane or interfering with prosthesis placement. However, it can also present opportunities in reconstructive surgery, potentially serving as a graft or vascularized flap for specific procedures.
Surgical Implications
In the case herein reported, the sternalis muscle was identified during the creation of the prosthesis pocket. This underscores the importance of flexibility in surgical planning and execution, particularly in procedures involving the anterior thoracic wall.
Failure to recognize the sternalis muscle intraoperatively could lead to unintended damage, increased complications, or suboptimal results. Surgeons must be prepared to identify such variants, as demonstrated in the case herein reported, in which adjustments ensured the successful completion of the procedure without compromising esthetic outcomes or patient safety.
In submuscular or dual-plane breast implant techniques, the sternalis muscle, if confidently identified, can provide additional coverage over the implant, enhancing overall cosmesis. However, caution must be taken to ensure the sternalis muscle is separated from its inferior sternal and costal attachments, so that it can lie tension-free over the implant. This step is critical to optimize blood flow to the pectoralis major muscle and prevent ischemia.7
If the sternalis is not adequately released, its longitudinal fibers may form a tight band over the medial portion of the pectoralis major muscle. This can result in compression of the pectoralis major between the sternalis muscle and the breast implant, increasing the risk of tissue ischemia.8
Moreover, in the presence of the sternalis muscle, the pectoralis major muscle is often medially deficient, leading to a smaller and more laterall-positioned implant pocket. To address this issue and achieve optimal implant positioning, the sternalis muscle should be incorporated into the horizontal dissection.7
Imaging Considerations
The sternalis muscle is also clinically significant in diagnostic imaging. It may mimic soft-tissue masses or pathological findings on mammography, computed tomography, or magnetic resonance imaging, leading to unnecessary investigations or interventions.9 Awareness of this variant among radiologists and clinicians is crucial to avoid misdiagnosis. Preoperative imaging that identifies the muscle can inform surgical planning and prevent intraoperative challenges.
Broader Implications
While the sternalis muscle remains a rare finding, its occasional identification should prompt surgeons and anatomists to deepen their understanding of anatomical variants. Incorporating this knowledge into training and clinical practice can improve outcomes across multiple disciplines, including breast surgery, thoracic surgery, and imaging.
Future Directions
The case herein reported adds to the growing body of literature on the sternalis muscle and its clinical relevance. Future studies should aim to: investigate the muscle’sprevalence in larger and more diverse populations, explore its potential usefulness in reconstructive or esthetic surgeries, and develop imaging protocols to better identify and document this variant preoperatively.
The case herein reported underscores the need for continued anatomical education and vigilance during surgical procedures. Recognizing the sternalis muscle ensures the achievement of surgical goals while respecting patient anatomy, paving the way for better outcomes and advancing the understanding of rare anatomical variations.
The sternalis muscle, while rare, represents a clinically-significant anatomical variant that surgeons should be prepared to encounter, especially during procedures involving the anterior thoracic wall, such as augmentation mastopexy. Its identification during the case herein reported underscores the importance of anatomical awareness and adaptability in the surgical practice.
The current report demonstrates that careful identification and preservation of the sternalis muscle during surgery do not compromise the procedure’s esthetic or functional outcomes. Adjustments in the technique enabled the seamless incorporation of the muscle into the surgical plan, ensuring the patient experienced a complication-free recovery, with excellent results.
The clinical significance of the sternalis muscle extends beyond surgery. Its potential to mimic pathological findings on imaging highlights the need for radiologists to be familiar with this variant to avoid misdiagnosis. Furthermore, its presence may offer reconstructive opportunities in specific cases, adding value to its recognition in clinical settings.
Future research should aim at expanding our understanding of the sternalis muscle, including its prevalence, embryological development, and potential applications in reconstructive surgery. By continuing to document such cases and increasing awareness among clinicians, we can enhance patient safety, optimize surgical outcomes, and deepen our knowledge of anatomical variations.
REFERENCES
1. Zielinska N, Pośnik M, Koptas K, Triantafyllou G, Moryś J, Olewnik Ł. Accessory thoracic muscles in human foetuses. Folia Morphol (Warsz) 2024;83(03):700–706. Doi: 10.5603/fm.99982
2. Asghar A, Naaz S, Narayan RK, Patra A. The prevalence and distribution of sternalis muscle: a meta-analysis of published literature of the last two hundred years. Anat Sci Int 2022;97(01): 110–123. Doi: 10.1007/s12565-021-00632-9
3. Raikos A, Paraskevas GK, Yusuf F, Kordali P, Ioannidis O, Brand-Saberi B. Sternalis muscle: a new crossed subtype, classification, and surgical applications. Ann Plast Surg 2011;67(06):646–648. Doi: 10.1097/SAP.0b013e31820d688b
4. Ramakrishnan S, Mahajan I, Nikitha T, Fernandez RK, Pillay M. An X across the Chest: A Rare Case of a Criss-crossed Sternalis Muscle. Acta Med Acad 2024;53(01):102–105. Doi: 10.5644/ama2006124.420
5. Li ASR, Sue M, Lombardi P, Bola HS, Bentley DC. Bilateral Sternalis Muscles: The Clinical Significance of This Rare Discovery. Cureus 2024;16(05):e60507. Doi: 10.7759/cureus.60507
6. Bahgat M, Khan AS, Alsemeh AE. Sternalis Muscle: A Cadaveric Case Report of a Rare Variant With Multiple Branching. Cureus 2024;16(08):e68263. Doi: 10.7759/cureus.68263
7. Slater J, McLean NR, Youssef M, Bristow G. Bilateral musculus sternalis -An anatomical and clinical review. Surgeon 2022;20 (06):e378–e381. Doi: 10.1016/j.surge.2021.12.011
8. Wynn J, Cole J, Scott S, Koo E. The sternalis muscle: an anatomical variant with clinical relevance for the breast and reconstructive surgeon. ANZ J Surg 2023;93(12):2999–3000. Doi: 10.1111/ans.18658
9. Bradley FM, Hoover HC Jr, Hulka CA, et al. The sternalis muscle: an unusual normal finding seen on mammography. AJR Am J Roentgenol 1996;166(01):33–36. Doi: 10.2214/ajr.166.1.8571900
1. Department of Plastic Surgery, Santa Maria di Leuca Clinic, Rome, Italy
2. Department of Surgical Sciences, University of Rome Tor Vergata, Rome, Italy
Data Availability
Financial Support The authors declare that they did not receive financial support from agencies in the public, private or nonprofit sectors to conduct the present study.
Address for correspondence Riccardo Foti, Dipartimento di Scienze Chirurgiche, Università degli Studi di Roma Tor Vergata, Roma, Italy (e-mail: riccardofoti.md@gmail.com).
Article received: August 29, 2025.
Article accepted: November 24, 2025.
Conflict of interests The authors have no conflict of interests to declare.
Editor-in-Chief: Dov Charles Goldenberg.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket