



Case Report - Year 2026 - Volume 41Issue 1
Burn Risks in Postabdominoplasty Patients: A Case Report
Riscos de queimaduras em pacientes após abdominoplastia: Relato de caso

ABSTRACT
A 34-year-old woman sustained a severe infraumbilical burn 2 years after undergoing abdominoplasty, caused by the use of a hot water bottle for menstrual pain relief. Due to persistent postoperative sensory loss in the lower abdomen-a common complication of abdominoplasty resulting from nerve disruption-she did not perceive the injury at the time. The burn led to extensive tissue damage and required prolonged healing by secondary intention. This case highlights the potential for unnoticed injuries in desensitized regions and the importance of thorough patient education regarding sensory deficits after abdominoplasty. Patients should be cautioned against using heat sources or engaging in activities that could harm insensate skin. While some degree of sensory recovery is expected, full restoration is not guaranteed, making preventive counseling essential. This case underscores the importance of thorough patient education on postoperative sensory changes and lifestyle adjustments to prevent potentially severe injuries.
Keywords: abdominoplasty; body contouring; burn; nerve injury
RESUMO
Uma mulher de 34 anos sofreu uma queimadura grave na região infraumbilical 2 anos após se submeter a uma abdominoplastia. A queimadura foi causada pelo uso de uma bolsa de água quente para alívio de dormenstrual. Devido à perda sensorial persistente no abdome inferior no período pós-operatório, uma complicação comum da abdominoplastia e decorrente de lesão nervosa, a paciente não percebeu a lesão à época. A queimadura provocou danos teciduais extensos e exigiu cicatrização prolongada por segunda intenção. Este caso destaca a possibilidade de lesões despercebidas em regiões dessensibilizadas e a importância da orientação completa do paciente sobre os déficits sensoriais após a abdominoplastia. Os pacientes devem ser alertados para não usar fontes de calor ou participar de atividades que possam lesionar a pele insensível. Embora algum grau de recuperação sensorial seja esperado, seu restauro completo é incerto, de modo que o aconselhamento preventivo é essencial. Este caso ressalta a importância da orientação completa do paciente sobre as alterações sensoriais após a cirurgia e os ajustes no estilo de vida para prevenir lesões potencialmente graves.
Palavras-chave: abdominoplastia; contorno corporal; queimaduras; lesão nervosa
Introduction
Abdominoplasty is one of the most common procedures in plastic surgery, aimed at treating excess skin, muscle laxity, and rectus muscle diastasis. The procedure involves lifting the skin flap, performing muscle plication, repositioning the umbilicus (by transposing it or sectioning it at its base), all of which impact the innervation of the anterior abdominal wall.
Despite its popularity and overall safety, the procedure is not without risks. Complications such as infection, bleeding, and poor wound healing are well-documented, with certain factors—such as obesity, smoking, and diabetes mellitus— significantly increasing these risks.1,2 However, a less-frequently discussed and underexplored complication of abdominoplasty is nerve injury. Nerve interruption during surgery may result in altered sensation in the treated areas, particularly in the infraumbilical region.
Postabdominoplasty nerve injuries can arise from two primary mechanisms: those caused by the surgical incision itself and those resulting from surgical positioning during the procedure. Notably, injuries to the lateral femoral cutaneous and iliohypogastric nerves have been identified as risks associated with the abdominoplasty incision.
This sensory impairment, even when temporary, increases the risk of burns in patients using heat sources, as they may not perceive excessive heat and are unable to prevent thermal damage to the skin.
Case Report
A female patient had undergone, 2 years earlier, a lipoabdominoplasty with correction of postpregnancy diastasis of the rectus muscles. The postoperative course was uneventful, and the patient was satisfied with the result.
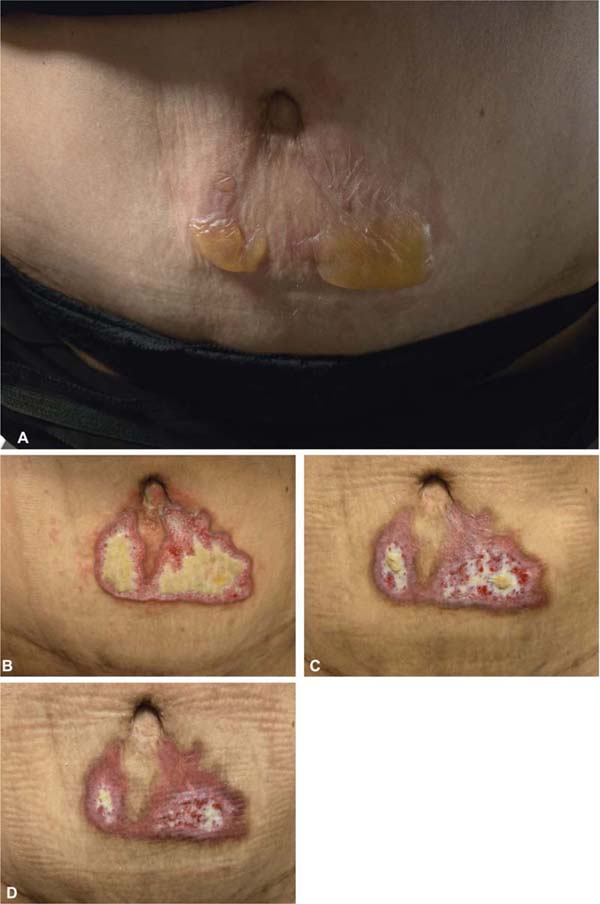
Due to menstrual pain, the patient took a painkiller and applied a hot-water bottle for a few minutes, over her shirt, in the lower abdomen. As the pain improved, the patient returned to her usual routine. In the evening, removing her clothing, the patient noticed red skin and the presence of blisters, even though she had not had any problems, nor pain during the day. In the following days, the patient noticed worsening in the region and sought medical care. After an initial surgical debridement, daily dressings with collagenase and paraffin gauze were recommended (►Fig. 1). After approximately 30 days of treatment, the patient healed.

Discussion
Nerve injury during surgery can occur through various mechanisms, including direct mechanical damage (caused by instruments such as a scalpel, suture, or cautery), indirect neuropathy (resulting from nerve entrapment within scar tissue formed during the procedure), or indirect compression neuropathy (arising from tissue edema around a nerve confined within a rigid or restricted anatomical space).3
One of the stages of abdominoplasty involves the elevation of the abdominal flap, which may extend up to the costal margin and temporarily or permanently disrupt superficial cutaneous innervation.
Innervation of the Anterior Abdominal Wall
The anterior abdominal wall is innervated by an intricate network of intercostal nerves (T7 through T12), the iliohypogastric nerve, and the ilioinguinal nerve (L1), which extend from the lower spine horizontally across the abdominal wall toward the midline (►Fig. 2). These nerves contribute to cutaneous sensation and to thermal and pain sensitivity (►Table 1).
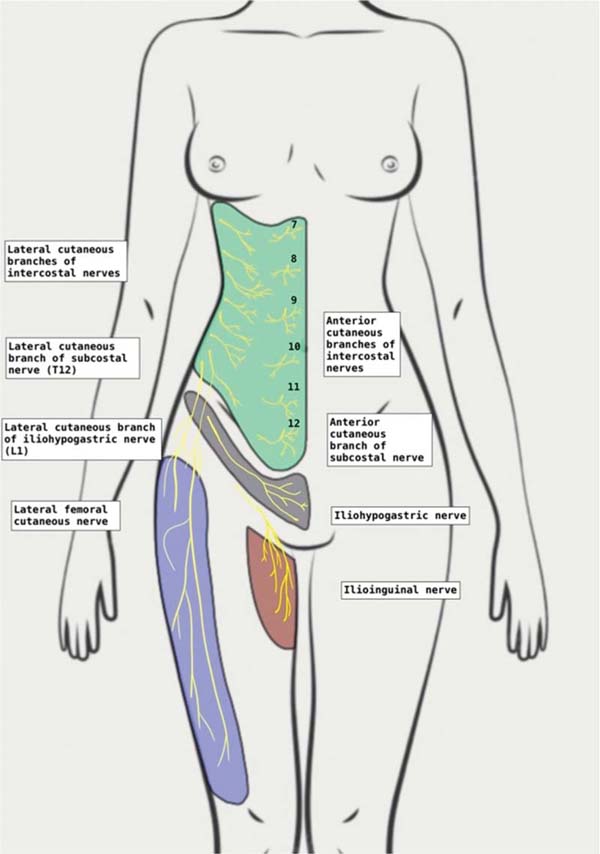

| Intercostal nerves (T7–T11) | These nerves emerge from the lower thoracic spine and travel laterally across the abdominal wall, branching into the superficial skin layers. They innervate the upper abdomen, including areas above and around the umbilicus. |
| Subcostal nerve (T12) | The subcostal nerve primarily innervates the lower abdominal region, including the infraumbilical region, which is particularly susceptible to sensory loss following abdominoplasty due to the extensive dissection. |
| Iliohypogastric nerve (L1) | The iliohypogastric nerve arises from the first lumbar nerve and divides into lateral and anterior branches. The lateral branch supplies the skin over the iliac crest, while the anterior branch innervates the skin of the suprapubic region. It has reciprocal relationship with the ilioinguinal neve, and they often communicate. |
| Ilioinguinal nerve (L1) | The ilioinguinal nerve also originates from the first lumbar nerve, and it provides sensory innervation to the skin of the upper medial thigh, mons pubis, and anterior part of the labia majora or scrotum. It also presents some overlap with the iliohypogastric nerve in its innervation zones. |
| Lateral femoral cutaneous nerve (L2–L3) | Although primarily a nerve of the thigh, the lateral femoral cutaneous nerve is of relevance during abdominal surgeries, as it courses near the anterior superior iliac spine. It provides sensory innervation to the skin of the lateral thigh and is at risk of injury during lower abdominal wall surgeries. This nerve is particularly vulnerable during surgical incision or retraction. Damage to this nerve can result inmeralgia paresthetica, which is characterized by pain, numbness, or burning sensations along the anterolateral thigh. It is the nerve most commonly injured after abdominoplasty. |

Burn Risks: Clinical Implications and Mechanisms of Thermal Injury
Postoperative thermal sensory loss represents a significant risk. Hot-water bottles, commonly used to alleviate abdominal or muscular pain, were shown4 to retain heat over 50 °C for at least 3 hours, which is sufficient to cause first-or second-degree burns within minutes. Under normal conditions, the cutaneous nervous system signals when the skin is exposed to excessive temperatures. However, in postabdominoplasty patients with reduced sensitivity, the ability to detect heat is compromised, especially in the infraumbilical region. This can lead to unrecognized burns until thermal damage has already occurred, potentially manifesting as erythema, blistering, or, in severe cases, necrosis of the superficial tissues.
Studies on Cutaneous Sensitivity Recovery
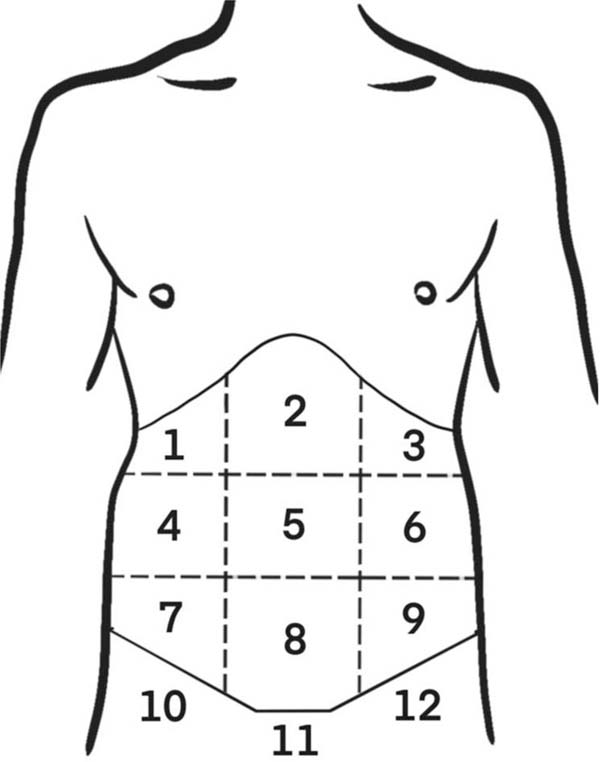
Studies conducted by Farah et al.5 aimed at evaluating sensory changes in the abdominal skin following abdominoplasty, using tests that simulated tactile, thermal, and pain sensitivity in common scenarios. The abdominal region was divided into 12 areas (►Fig. 3). Their findings revealed that the most significant decrease in sensitivity occurred in area 8, which also showed diminished pressure sensitivity. While area 11 exhibited a statistically significant reduction in hot and cold temperature sensitivity, the changes were less pronounced than those observed in area 8. These results align with anatomical considerations, as the anterior cutaneous nerves—which are responsible for supplying the abdominal wall—are severed during the undermining of the abdominal flap, particularly affecting the hypogastric region (area 8). This area becomes the distal-most point of sensitive nerve connections after surgery, as the extensive incision and undermining isolate it from adjacent nerve supply. Conversely, the suprapubic region (area 11) likely experiences sensory loss due to traction rather than nerve disruption, as undermining is not typically performed in this region. These patterns of sensory change emphasize the distinct mechanisms influencing nerve injury in different abdominal areas. Supporting these findings, research on skin flaps suggests that sensory recovery follows a predictable sequence, with pain returning first, followed by tactile, and, finally, thermal sensitivity. Understanding these dynamics is crucial for surgeons aiming at minimizing sensory loss and optimizing postoperative outcomes in abdominoplasty patients.

While most patients experience partial sensation recovery within months after surgery, some may have long-term hypoesthesia or anesthesia, leaving the area vulnerable to thermal trauma, especially if they use heating devices like hot-water bottles.
The scientific literature suggests that postabdominoplasty sensory loss follows a variable recovery pattern. While most patients experience partial sensory recovery within 6 to 12 months,6 full restoration is not guaranteed. Studies7 indicate that nerve damage can lead to long-lasting neuropathies, with thermal sensitivity being one of the most challenging sensations to regain. In fact, after a period in which subjects perceive no stimuli at the flap, pain sensation returns first, followed by tactile, and, finally, thermal sensibility.
Literature Review on Postabdominoplasty Burns
Burn injuries in patients following abdominoplasty, particularly from hot-water bottles or other heat sources, have only been reported in a few other cases.8 These incidents highlight the vulnerability of postoperative patients to thermal injuries due to compromised cutaneous sensation, particularly in the infraumbilical region.
In 2023, Alokaili et al.9 reported the case of a 26-year-old healthy female post-abdominoplasty patient who sustained an incidental contact burn injury caused by the use of a common home remedy for menstrual pain. In this instance, the burn healed via secondary intention.
In early 2024, Syras et al.10 documented 3 cases of third-degree contact burns at the infraumbilical level, resulting from the use of a hot-water bottle shortly after abdominoplasty. These injuries led to significant esthetic sequelae.
Both studies recommend counseling patients regarding caution or the avoidance of such practices following abdominoplasty, particularly given the potentially-disfiguring complications associated with thermal injuries.
Abdominoplasty inevitably leads to temporary or permanent reductions in cutaneous sensitivity in the infraumbilical region, with significant implications for patient safety. The risk of burns from the application of hot-water bottles is high and requires careful preventative management, including detailed preoperative education and continuous postoperative monitoring. A thorough knowledge of anatomy and anatomical variations helps prevent injuries, butahigh index ofsuspicion should be maintained to accurately diagnose nerve injuries in patients presenting with chronic postoperative pain or apparent nerve dysfunction. Given the temporary or permanent hypoanesthesia of the infraumbilical region following abdominoplasty, the literature consistently emphasizes the importance of patient education regarding the altered sensory landscape postoperatively, particularly in relation to heat-application risks. Ensuring patients understand the risks and adopt preventative measures can significantly reduce the likelihood of thermal injuries, enhancing postoperative recovery and overall patient experience.
REFERENCES
1. Vastine VL, Morgan RF, Williams GS, et al. Wound complications of abdominoplasty in obese patients. Ann Plast Surg 1999;42(01): 34–39. Doi: 10.1097/00000637-199901000-00006
2. Araco A, Gravante G, Sorge R, Araco F, Delogu D, Cervelli V. Wound infections in aesthetic abdominoplasties: the role of smoking. Plast Reconstr Surg 2008;121(05):305e–310e. Doi: 10.1097/PRS.0b013e31816b13c2
3. Ducic I, Zakaria HM, Felder JM III, Arnspiger S. Abdomino-plasty-related nerve injuries: systematic review and treatment options. Aesthet Surg J 2014;34(02):284–297. Doi: 10.1177/1090820X13516341
4. Goltsman D, Li Z, Bruce E, et al. Too hot to handle? Hot water bottle injuries in Sydney, Australia. Burns 2015;41(04):770–777. Doi: 10.1016/j.burns.2014.10.025
5. Farah AB, Nahas FX, Ferreira LM, Mendes JdeA, Juliano Y. Sensibility of the abdomen after abdominoplasty. Plast Reconstr Surg 2004;114(02):577–582, discussion 583. Doi: 10.1097/01.prs.0000128356.93462.7b
6. Aherrera AS, Pincus DJ, Vernadakis AJ, Pandya SN. Evaluation of abdominal cutaneous sensibility following abdominoplasty. Plast Reconstr Surg 2015;135(03):526e–532e. Doi: 10.1097/PRS.0000000000000969
7. Woodward KL, Kenshalo DR Sr. The recovery of sensory function following skin flaps in humans. Plast Reconstr Surg 1987;79(03): 428–435. Doi: 10.1097/00006534-198703000-00021
8. Ozgenel Ege GY, Ozcan M. Heating-pad burn as a complication of abdominoplasty. Br J Plast Surg 2003;56(01):52–53. Doi: 10.1016/s0007-1226(03)00014-6
9. Alokaili H, Hanawi M, Aldaker F, et al. Dysmenorrhea Heat Therapy Injury in a Post-Abdominoplasty Patient: A Case Report. Cureus 2023;15(06):e40169. Doi: 10.7759/cureus.40169
10. Syras C, Lacroix G, Guerreschi P, Dumont A, Pasquesoone L. [CONTACT BURNS WITH A HOT WATER BOTTLE FOLLOWING AN ABDOMINOPLASTY. CASE REPORTS AND LITERATURE REVIEW.]. Ann Burns Fire Disasters 2024;37(02):101–105
1. Private Practice, Casa di Cura Santa Maria di Leuca, Roma, RM, Italy
2. Plastic and Reconstructive Surgery Service, Department of Surgical Sciences, School
of Medicine and Surgery, Università degli Studi di Roma Tor Vergata, Rome, RM, Italy
3. Università Degli Studi di Roma La Sapienza, Roma, RM, Italy
Data Availability
Financial Support The authors declare that they did not receive financial support from agencies in the public, private or non-profit sectors to conduct the present study.
Address for correspondence Riccardo Foti, Settore di Chirurgia Plastica e Ricostruttiva, DipartimentodiScienze Chirurgiche, Facoltá di Medicina e Chirurgia, Università degli Studi di Roma Tor Vergata, Roma, 00133, Italy (e-mail: riccardofoti.md@gmail.com).
Article received: September 01, 2025.
Article accepted: November 24, 2025.
Conflict of Interests The authors have no conflict of interests to declare.
Editor-in-Chief: Dov Charles Goldenberg.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket