



Original Article - Year 2026 - Volume 41Issue 1
Prospective Study of Burn Admissions in Rio Grande do Norte: Incidence, Complications, and Patient Profile
Estudo prospectivo das internações por queimaduras no Rio Grande do Norte: incidência, complicações e perfil dos pacientes
Bárbara Xavier Gomes da Silva1, ; Juan Braga Lousada Vidal1; Samuel Maia Lira1; Sara Thalya Santos Ferreira1; Pedro Ricarte Cândido Dantas1; Marco Antônio Martins Ribeiro de Almeida2; Eveline Pipolo Milan3; Henrique de Paula Bedaque4
; Juan Braga Lousada Vidal1; Samuel Maia Lira1; Sara Thalya Santos Ferreira1; Pedro Ricarte Cândido Dantas1; Marco Antônio Martins Ribeiro de Almeida2; Eveline Pipolo Milan3; Henrique de Paula Bedaque4
ABSTRACT
Introduction Burns are highly prevalent injuries in Brazil. These injuries may have severe complications, making their treatment complex. Sequelae are mostly permanent and result in physical, psychological, and economic losses. Despite the relevance of epidemiological data for improving care and guiding preventive actions, burns are not a notifiable disease, and there are no previous studies on hospitalizations at the Burn Treatment Center of Hospital Monsenhor Walfredo Gurgel (Centro de Tratamento de Queimados do Hospital Monsenhor Walfredo Gurgel, CTQ-HMWG, in Portuguese), the only referral service in Rio Grande do Norte, Brazil.
Objective To describe the epidemiological profile andmain complications of patients admitted to CTQ-HMWG between November 2023 and November 2024.
Materials and Methods The present prospective and analytical study collected epidemiological and clinical data from patients admitted to CTQ-HMWG between November 2023 and November 2024. These data included interviews with patients or their legal guardians, as well as information from medical records.
Results Eighty patients were analyzed, predominantly mixed-race men with no formal education and of working age. Burns occurred mainly in domestic settings, with scalds being the most frequent cause, followed by flammable fluids and electrical accidents. The most prevalent complications were wound infection and sepsis.
Conclusion The study highlights the social and economic impact of burns in the state, reinforcing the need for public policies focused on prevention, home and workplace safety, as well as the expansion of ongoing educational strategies, to reduce morbidity and mortality and improve the quality of life of victims.
Keywords: Brazil; statistics on sequelae and disability; health profile; burns; burn unit
RESUMO
Introdução As queimaduras são lesões de alta incidência no Brasil, comelevado potencial de complicações graves, o que torna seu tratamento complexo. As sequelas, em grande parte permanentes, geram prejuízos físicos, psicológicos e econômicos. Apesar da relevância dos dados epidemiológicos para aprimorar a assistência e orientar ações preventivas, as queimaduras não constituem agravo de notificação compulsória, e não há estudos prévios sobre internações no Centro de Tratamento de Queimados do Hospital Monsenhor Walfredo Gurgel (CTQ-HMWG), único serviço de referência no Rio Grande do Norte.
Objetivo Descrever o perfil epidemiológico e as principais complicações dos pacientes internados no CTQ-HMWG entre novembro de 2023 a novembro de 2024.
Materiais e Métodos Estudo prospectivo e analítico, com coleta de dados epidemiológicos e clínicos de pacientes internados no CTQ-HMWG entre novembro de 2023 e novembro de 2024, obtidos por meio de entrevistas com os próprios pacientes ou responsáveis legais, complementados por informações de prontuário.
Resultados Foram analisados 80 pacientes, predominando homens pardos, sem escolaridade formal, em idade economicamente ativa. As queimaduras ocorreram principalmente em ambiente doméstico, sendo as escaldaduras o agente mais frequente, seguidas por líquidos inflamáveis e acidentes elétricos. As complicações mais prevalentes foram infecção da ferida e sepse.
Conclusão O estudo evidencia o impacto social e econômico das queimaduras no estado, reforçando a necessidade de políticas públicas voltadas à prevenção, segurança doméstica e laboral, além da ampliação de estratégias educativas permanentes, a fim de reduzir a morbimortalidade e melhorar a qualidade de vida das vítimas.
Palavras-chave: Brasil; estatísticas de sequelas e incapacidade; perfil de saúde; queimaduras; unidade de queimados
Introduction
The World Health Organization (WHO) estimates that approximately 11 million subjects sustain burn injuries each year, resulting in around 180,000 deaths worldwide. Regardless of etiology, burns are complex injuries that are difficult to treat and are associated with high morbidity and mortality rates. Recovery is not achieved solely through wound healing, as burn injuries lead to profound and long-term physical, psychological, and social consequences requiring addressing to optimize patients’ quality of life.1,2
Burns mostly occur at home due to lapses in attention to household hazards.3 In Brazil, approximately 1 million people suffer burns annually, but only about 100 thousand of them seek medical assistance. These injuries result in approximately 2,500 deaths per year, both from direct and indirect burn consequences.4 Furthermore, according to information from the Brazilian Unified Health System (Sistema Único de Saúde, SUS, in Portuguese), approximately 30,000 people are hospitalized annually due to this type of injury.5
Therefore, prevention is a priority, as burns are severe yet potentially preventable injuries. As such, it is possible to mitigate them with epidemiological principles, awareness campaigns, and effective educational programs.6–8 Epidemiology is fundamental to formulate public health policies, as it provides essential data for the evaluation and development of treatment strategies and prevention initiatives, while also contributing to the identification and understanding of underlying causal factors. However, epidemiological studies addressing burn injuries remain scarce in Brazil.
Epidemiological data from Brazilian burn units allow healthcare institutions to determine the demand for beds by geographic region, as well as outcome parameters, length of stay, bed occupancy, mortality and infection rates, and use of materials, including antibiotics, blood products, and tem-porary skin substitutes—essential information for improving administrative planning, treatment, and rehabilitation of burn patients.9
According to the Brazilian Burn Society (Sociedade Brasileira de Queimaduras, SBQ), Brazil has 83 registered Burn Treatment Units (BTUs).10 These units are specialized centers for treating patients with complex second-and third-degree burns, often associated with significant comorbidities. They are multidisciplinary treatment centers, where dozens of professionals provide specialized care to patients.11
The state of Rio Grande do Norte (RN), in Northeastern Brazil, has a single specialized burn treatment center—the Burn Treatment Center of Hospital Monsenhor Walfredo Gurgel (Centro de Tratamento de Queimados do Hospital Monsenhor Walfredo Gurgel, CTQ-HMWG, in Portuguese)— to provide care for approximately 3 million inhabitants of the state.12 Although epidemiological data are essential for prevention strategies, improvements in care processes, and the formulation of public policies, hospitalization data in Brazil are primarily derived from the SUS Hospital Information System (Sistema de Informações Hospitalares, SIH/SUS, in Portuguese), which is structured for institutional reimbursement purposes. Consequently, SIH/SUS lacks detailed information on individual patients, burn circumstances, and trauma severity. Since data are aggregated rather than patient-specific, prognostic analyses and more in-depth clinical and epidemiological characterization of patients treated at this center are not feasible.5,12
Objectives
The overall objective of the present study was to analyze the clinical and epidemiological profile of patients admitted to CTQ-HMWG from November 2023 to November 2024, considering sociodemographic aspects such as sex, age, race, schooling level, professional occupation, and origin, as well as the etiology, extent, and severity of injuries, including burned body surface area, affected locations, and smoke inhalation. In addition, the study aimed to identify burn circumstances, differentiating between accidental situa-tions, violence, or attempted suicide, as well as analyzing the occurrence of associated traumas, clinical complications during hospitalization, length of stay in the ward and intensive care unit (ICU), and clinical outcomes.
Methods
The present analytical, prospective, and qualitative-quantitative study included severely burned patients admitted to CTQ-HMWG in the state of Rio Grande do Norte, Brazil, between November 2023 and November 2024. These patients presented with one of the following characteristics: 2nd-degree burns affecting 20% or more of the body surface area, 3rd-degree burns involving 10% or more of the body surface area, perineal burns, smoke inhalation injury, poly-trauma, head trauma, electrical trauma, shock, renal failure, heart failure, liver failure, hemostasis disorders, pulmonary embolism, acute myocardial infarction, severe infectious conditions resulting from the burn or unrelated it, compartment syndrome, and wasting diseases. The Research Ethics Committee of the Onofre Lopes University Hospital approved this study under opinion number 6.466.340.
Only patients or caregivers who refused to sign the informed consent form (ICF) and/or informed assent form (IAF) were excluded. For patients unable to respond to the survey, such as those under orotracheal intubation or with a decreased level of consciousness, their caregivers signed the ICF and provided information for the study. When the patient was able to respond to the questionnaire again, they were approached to sign the ICF and confirm information. Patients without caregivers throughout the hospitalization period and/or lacking autonomous capacity were excluded from the study.
All patients admitted to CTQ-HMWG were invited to participate in the study. Patients received a detailed explanation of the study methodology in clear and appropriate language, including potential benefits and possible risks. It was emphasized that participation in the study was voluntary and that refusal to participate would not compromise access to the best available care.
The sample was selected by convenience, including all patients who agreed to participate after the procedures mentioned in the preceding paragraph, thereby maximizing the number of potential participants.
Data was collected through interviews with research participants and/or the guardians of minors who had signed the informed consent forms. When necessary, interview data were supplemented by information provided by health professionals working at CTQ-HMWG and by medical record review to obtain clinical variables (e.g., packed cell volume [PCV] and hemoglobin levels) or information that patients were unable to report. Moreover, medical records were essential for the exploratory analysis of injury circumstances and complications, as they enabled longitudinal monitoring of patient outcomes within the service.
Collected data (variables) included sex, date of birth, race, schooling level, professional occupation, and city of origin, to identify the sociodemographic characteristics of patients most affected by burns and thus generate hypotheses about their main causal and regional factors. Etiology, burned body surface area, affected anatomical sites, and special burn-related factors—such as smoke inhalation—are key variables for assessing injury cause, extent, and severity, which are critical for predicting patient morbidity and mortality. Data on burn location, context, and concomitant traumas are essential to formulate hypotheses about trauma circumstances and causal effects to develop preventive measures for the general population. Length of hospital stay, complications, and outcomes provide an overview of complications, mostly wound infection, sepsis, septic shock, pneumonia, endotra-cheal intubation, tracheostomy, urinary tract infection, amputation, deep vein thrombosis (DVT), and pressure ulcers. These data were correlated with burn circumstances, patient clinical progression, and admission period. Packed-cell volume and hemoglobin levels at admission were considered key indicators for evaluating patients’ biochemical status in relation to these characteristics.
Accordingly, burn etiology, severity, and context were analyzed, along with length of hospital stay and the occurrence of sepsis, amputation, intubation, and other complications. Clinical and complementary data were entered into a Microsoft Excel for Windows (Microsoft Corp.) database, from which the required analyses were performed.
The quantitative variables age, hemoglobin levels, and PCV at admission were assessed for normality using the Shapiro-Wilk test. Among these variables, only age did not present a normal distribution. Results were described using absolute and relative frequencies, means, and medians, and were presented in tables and graphs to facilitate visualization of data distribution.
Results
Data from 80 patients were collected between November 2023 and August 2024, as described in ► Table 1. The most predominant age range was from 18 to 60 years old, followed by those under 18 years old. The average age was 26.5 years.
| Characteristic | n | % |
|---|---|---|
| Sex | ||
| Male | 45 | 56 |
| Female | 35 | 44 |
| Age group | ||
| 0–12 years | 27 | 34 |
| 13–17 years | 4 | 5 |
| 18–60 years | 36 | 45 |
| > 60 years | 13 | 16 |
Note: Distribution of patients by sex and age group from Novem-ber 2023 to August 2024. Source: Burn Treatment Center of Hospital Monsenhor Walfredo Gurgel (Centro de Tratamento de Queimados do Hospital Monsenhor Walfredo Gurgel, CTQ-HMWG, in Portuguese).

Regarding race, 45 patients (56%) were classified as brown, 18 (23%) as White, 16 (20%) as Black, and 1 (1%) as Asian. With respect to schooling level, most patients had no formal education (n ¼ 50; 63%), followed by those who had completed primary education (n ¼ 19; 24%), secondary education (n ¼ 9; 11%), and higher education (n ¼ 2; 3%).
The predominant causes of burns were scalds, followed by flammable fluids and electricity (► Table 2). Injuries from flames and chemical agents were less common. Burns caused by contact with heated surfaces had a mean burned body surface area of 16.86%.
| Etiology | n | % |
|---|---|---|
| Scalding | 22 | 28 |
| Flammable fluids | 20 | 25 |
| Electricity | 17 | 21 |
| Flames | 12 | 15 |
| Hot surfaces | 8 | 10 |
| Chemical agents | 1 | 1.25 |
Note: Distribution of burn causes among patients treated at the Burn Treatment Center of Hospital Monsenhor Walfredo Gurgel (Centro de Tratamento de Queimados do Hospital Monsenhor Walfredo Gurgel, CTQ-HMWG, in Portuguese) from November 2023 to August 2024. Source: CTQ-HMWG.

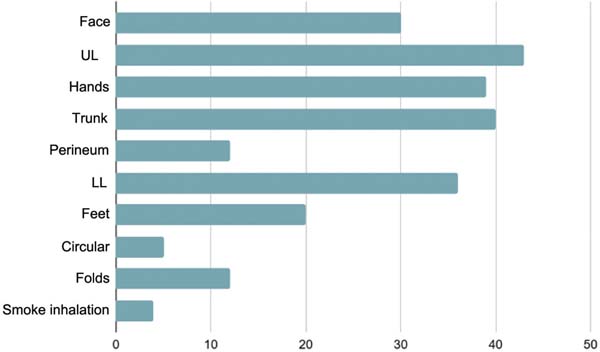
The distribution of burn-affected anatomical sites was broad, with the highest incidence in the upper limbs (43 cases; 53.75%), followed by the trunk (40 cases; 50%) and the hands (39 cases; 48.75%). Facial burns were observed in approximately one-third of cases (37.5%), while the lower limbs and feet were involved in 45% and 25% of patients, respectively. In addition, areas such as the perineum, folds, and circular burns were affected to a lesser extent, with 12 (15%), 12 (15%), and 5 cases (6%), respectively. Smoke inhalation was a complication observed in 5% of patients (► Fig. 1).

The household environment was the primary setting in which burn injuries occurred, accounting for most cases, as detailed in ► Table 3. In workplaces and other environments, proportions were smaller. Most incidents were accidental, with a small number related to suicide attempts and one episode involving violence.
| Characteristic | n | % |
|---|---|---|
| Occurrence site | ||
| Household | 58 | 72.5 |
| Workplace | 13 | 16.25 |
| Other environments | 9 | 11.25 |
| Burn nature | ||
| Accident | 77 | 96 |
| Attempted suicide | 2 | 3 |
| Violence | 1 | 1 |
Source: Burn Treatment Center of Hospital Monsenhor Walfredo Gurgel (Centro de Tratamento de Queimados do Hospital Monsenhor Walfredo Gurgel, CTQ-HMWG, in Portuguese).

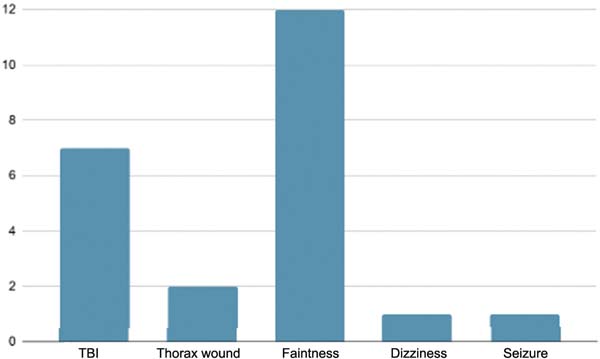
Furthermore, patients reported associated injuries occurring at the time of the burn, including episodes of fainting, traumatic brain injury (TBI), chest trauma, dizziness, and seizures, as detailed in ► Fig. 2. A subset of patients required admission to the ICU, with a mean ICU stay of 2.5 days. The overall mean length of hospital stay was 21.4 days.

The most prevalent complications during hospitalization were wound infection and sepsis, affecting 24 (30%) and 4 (5%) of the patients, respectively. Other complications, including urinary tract infection, escharotomy, anemia, amputation, colostomy, pleural effusion, phlebitis, and diarrhea, occurred in 3 or fewer patients.
Regarding admission laboratory data, the mean PCV was 36.6%, with a median of 35%. For hemoglobin levels, the mean value was 13.32 g/dL, with a median of 11.8 g/dL.
Taken together, these findings indicate that burn injuries represent a significant cause of external injury in Brazil, frequently resulting in profound and often irreversible physical, psychological, and social consequences. Beyond the physical sequelae associated with scarring, burns adversely affect multiple dimensions of life, including work, leisure, interpersonal relationships, religious participation, educational activities, and daily routines.13 In this context, investigating and understanding the epidemiology of burn injuries is essential as a fundamental tool for prevention and for reducing this substantial burden of morbidity, particularly given that epidemiological patterns vary according to geographic, temporal, cultural, social, and individual factors.14
In this study, the highest incidence of burns occurred in males, a fact that aligns with data from both Brazilian15 and international studies.16 This finding has multifactorial justifications, possibly related to cultural and occupational factors. Culturally, men have historically shown a greater tendency to take risky actions compared to women, who, in turn, demonstrate greater caution. Behavioral studies can corroborate this fact by indicating that, in domains such as health/safety, for instance, attitudes towards the coronavirus disease 2019 (COVID-19) pandemic, ethical issues, finances, and recreational activities, women report a lower probability of engaging in dangerous behaviors.8 In many occupational sectors, men are predominantly employed in professions involving greater physical risk, such as construction, mining, and heavy manufacturing. These occupations are associated with an increased risk of workplace accidents, including burn injuries.17
The most affected age group is between 18 and 60 years old (45%), representing a large part of the Brazilian econom-ically active population. This data reinforces the importance of investing in policies aimed at workplace safety and highlights the economic impact of burns, since the most affected group corresponds to the country’s main productive force. Next, the pediatric population, from 0 to 12 years old (34%), stands out. Children’s natural curiosity and exploratory behavior increase their vulnerability to burn injuries.18 This occurs because children’s intellectual and cognitive development does not keep pace with their motor development progress. Thus, the greater motor autonomy of children, combined with the difficulty in understanding cause and effect, can increase their vulnerability to burns.19 The lack of vigilance on the part of caregivers, who frequently need to divide their attention between parental care and other domestic or work activities, also contributes to child-ren’s exposure to risks. The elderly population (over 60 years old) accounts for 16% of those affected. This group deserves special attention because it presents greater hemodynamic instability, making burns potentially more severe, with a higher risk of complications and death.
Regarding racial epidemiology, there was a higher percentage of people who self-identified as brown (56%). Although racial self-identification is a personal choice, it is influenced deeply by the complex social dynamics of the country. It is worth noting that many people do not have a precise understanding of racial categories, and subjects who might identify as Black often prefer to declare themselves brown due to greater social acceptance and, in some cases, an attempt to avoid the stigma associated with Blackness.20 Historical factors, such as the whitening policies from the late nineteenth and early twentieth centuries, influenced the perception and valuation of racial identity, creating a tendency to prefer racially lighter identities, such as the “mixedrace” classification.
As for educational level, 63% of participants had no formal education, 23% had completed primary education, 11% had completed secondary education, and only 3% had completed higher education. Therefore, an inverse association was observed between educational level and burn incidence. Individuals with lower educational levels may have reduced access to information on domestic accident prevention and safety measures, as well as greater difficulty in recognizing and understanding risks associated with certain situations, such as improper use of household appliances or inadequate supervision of children in hazardous environments.21 These subjects are more frequently employed in occupations with higher burn risk—such as industrial kitchens, construction, factory work, or chemical handling—often without adequate access to personal protective equipment (PPE) or in settings where safety standards are insufficient. In addition, they are more likely to live in precarious housing conditions, with increased exposure to low-quality gas stoves, wood-burning stoves, or inadequate electrical systems.
The most common cause of burns was scalding (28%), consistent with other Brazilian studies.22 A potential explanation for this finding is the daily use of hot fluids in the home environment, such as boiling water, coffee, tea, soups, and cooking oils, which increases the risk of accidents. Furthermore, especially in less developed regions, many households do not adopt proper safety measures, such as stove protectors or positioning pots with the handles turned inwards. This factor is particularly relevant at the extremes of age. Children, due to their natural curiosity and increasing mobility, are more likely to come into contact with hot fluids, particularly given their height, which places them closer to surfaces such as tables and countertops where these substances can be easily accessed and spilled. Older adults, in turn, may experience reduced sensitivity and slower reflexes associated with aging, which can delay the perception of imminent danger and increase the risk of burn injuries.
Flammable fluids (25%) were the second leading cause of burns. Substances such as gasoline, alcohol, kerosene, and acetone have relatively low flash points, meaning they can easily ignite upon contact with a heat source, spark, or flame. These fluids release flammable vapors that can spread in the air and accumulate in enclosed areas, increasing the risk of ignition. In addition, these substances are commonly used in households for cleaning, fire ignition, and as fuel, often involving improper handling or unsafe storage practices.
Electricity (21%) ranks third as a cause of burns; in these cases, electric current can result in internal burns to tissues and organs, even when the skin appears relatively intact externally. Social and occupational factors are strongly associated with these burn injuries, as inadequate or defective electrical installations increase risk. Exposed wiring, overloaded circuits, poorly maintained electrical equipment, and the absence of regular maintenance of electrical systems all contribute to a higher likelihood of burns. The employment context should also be considered; workers may be exposed to electrical hazards due to the nature of their work, includ-ing handling large amounts of electrical energy without proper precautions, and failure to use PPE, such as insulating gloves and appropriate tools, can result in direct contact with electric currents. Most victims of electrical burns are young men, consistent with the observation that men experience more burns due to occupational exposure in high-risk sectors.23
As for distribution, most burns involved the upper limbs (43%), which is consistent with Brazilian studies.24 These data may be related to the person’s position relative to the flame source. The hands (39%) are the part of the body most used to manipulate objects and perform daily tasks; as a result, they are often the first to come into contact with heat sources, hot fluids, and other burn causes.
The household (72.5%) and work (16.25%) environments were the main locations for burn occurrence. In the household, the constant proximity to heat sources, such as stoves and heaters, and the frequency of activities involving heat (such as cooking) increase the risk of burns. This fact, combined with the lack of habit of using heat-resistant gloves or long sleeves during hazardous activities, can further elevate this risk. In industrial environments, workers are frequently exposed to burn hazards and may not consistently wear appropriate personal protective equipment for their activities.
The most frequently burn-associated trauma was fainting, with 12 cases, since the pain resulting from a burn can overstimulate the vagal system. The autonomic nervous system’s response leads to decreased blood pressure and reduced blood flow to the brain, causing fainting.25 TBIs were also frequent, with seven cases, potentially resulting from accident-induced panic, causing disorientation and/or loss of balance. In industrial or household environments, explosions involving flammable fluids, gases, or chemicals can cause both burns and TBI.
Packed-cell volume and hemoglobin levels are expected to increase in extensive burns due to the strong tissue necrosis, vigorous fluid loss, and vasodilation, leading to initial hemoconcentration. The main complications in burn patients were wound infection and sepsis. These factors occur because burns significantly disrupt the skin barrier, that is, the first line of defense against pathogens.26 Furthermore, extensive burns induce immunosuppression, increasing susceptibility to infections. Another factor is that burn patients also face a high risk of infections due to the presence of multidrugresistant organisms in burn units.27–30 Therefore, effective infection management in burn patients requires a multidisciplinary approach and the use of rigorous infection control measures.
Most burns were accidental (96%). Although burns are complex traumas requiring multidisciplinary and highly complex treatment, fortunately, it is possible to prevent them through awareness campaigns and greater dissemination of information to the population.
Conclusion
Burns constitute a significant public health problem, affecting different age groups and presenting both physical, psychological, and social implications. Understanding the epidemiological profile of this injury in Rio Grande do Norte allows not only the identification of the most vulnerable groups but also supports the formulation of effective preventive strategies.
The incidence of burns was higher in men of working age, followed by children and the elderly, confirming the vulnerability of extreme age groups. Low educational attainment, adverse working conditions, and cultural factors emerged as key determinants of vulnerability to burn injuries.
Regarding etiology, the main causes identified were scalds, flammable fluids, and electricity, with a predominance of accidents in the household environment. However, work-related cases, suicide attempts, and episodes of violence also occurred. Most injuries affected the upper limbs, hands, trunk, and face, and about 5% of patients presented with smoke inhalation, highlighting the severity of the occurrences.
Associated traumas included fainting, head and chest trauma, seizures, and dizziness. The most prevalent clinical complications were wound infection and sepsis, followed by urinary tract infection, anemia, and amputation, reflecting the complexity of clinical management. The overall average length of stay was 21.4 days, with some patients requiring ICU admission for an average stay of 2.5 days.
Clinical outcomes included hospital discharges, sequelae, and death, reinforcing the impact of burns on morbidity and mortality. Despite advances in clinical management and multidisciplinary care, prevention remains the primary strategy for reducing the incidence of burn injuries and minimizing their physical, psychological, and economic impacts.
Accordingly, this study reinforces the need for sustained educational campaigns, household and workplace safety programs, and the development of permanent public policies that expand access to information, protective resources, and rehabilitation services. Such measures are essential for reducing burn-related morbidity, mortality, and long-term sequelae, thereby improving the quality of life of affected patients and their families.
REFERENCES
1. Jeschke MG, Van Baar ME, Choudhry MA, Chung KK, Gibran NS, Logsetty S. Burn injury. Nat Rev Dis Primers 2020;6(01):11. Doi: 10.1038/s41572-020-0145-5
2. Synodinou D, Savoie-White FH, Sangone A, et al. Health utilities in burn injury survivors: A systematic review. Burns 2022;48(01): 13–22. Doi: 10.1016/j.burns.2021.09.003
3. Mehta K, Thrikutam N, Hoyte-Williams PE, Falk H, Nakarmi K, Stewart B. Epidemiology and outcomes of cooking-and cooks-tove-related burn injuries: A World Health Organization Global Burn Registry report. J Burn Care Res 2023;44(03):508–516. Doi: 10.1093/jbcr/irab166
4. Cunha CB, Campos RC, Azevedo TAM, Gianini VHA, Alves BB, Cavalheiro LT. Perfil clínico e epidemiológico de pacientes vítimas de queimaduras, um estudo retrospectivo. Rev Bras Cir Plást 2023;38. Doi: 10.5935/2177-1235.2023rbcp0730-pt
5. Instituto Brasileiro de Geografia e Estatística (IBGE) Sistema de Informações Hospitalares do SUS – SIH/SUS [Internet]. [Acessado em 12 ago. 2024]. Disponível em: https://ces.ibge.gov.br/base-de-dados/metadados/ministerio-da-saude/sistema-de-informa-coes-hospitalares-do-sus-sih-sus.html
6. Fontana TdS, Lopes LV, Linch GFdC, Paz AA, Souza EN. Queimaduras no Brasil: Análise retrospectiva de internações e mortalidade. Rev Bras Queimaduras 2020;19(01):65–71 Disponível em: https://www.rbqueimaduras.com.br/details/501/pt-BR/queimaduras-no-brasil–analise-retrospectiva-de-internacoes-e-mortalidade
7. Souza TG, Souza KM. Série temporal das internações hospitalares por queimaduras em pacientes pediátricos na Região Sul do Brasil no período de 2016 a 2020. Rev Bras Cir Plást 2022;37:634. Doi: 10.5935/2177-1235.2022rbcp-pt
8. Opriessnig E, Luze H, Smolle C, et al. Epidemiology of burn injury and the ideal dressing in global burn care -Regional differences explored. Burns 2023;49(01):1–14. Doi: 10.1016/j.burns.2022.06.018
9. Dias LDF, Oliveira AF, Juliano Y, Ferreira LM. Burn Care Unit of São Paulo Federal University: an epidemiological profile. Rev Bras Cir Plast 2015;30(01):86–92. Doi: 10.5935/2177-1235.2015RBCP0121
10. Sociedade Brasileira de Queimaduras (SBQ) A realidade dos CTQs pelo Brasil – Unidade de Tratamento de Queimados do Hospital de Urgência de Sergipe [Internet]. Goiânia: SBQ; 2021 [citado 14 jun. 2025]. Disponível em: https://sbqueimaduras.org.br/noticia/a-realidade-dos-ctqs-pelo-brasil–unidade-de-tratamento-de-queimados-utq-do-hospital-de-urgencia-de-sergipe
11. Sheridan R, Barillo D, Herndon D, et al. Burn specialty teams. J Burn Care Rehabil 2005;26(02):170–173. Doi: 10.1097/01.bcr.0000155544.38709.6e
12. Instituto Brasileiro de Geografia e Estatística (IBGE) Censo Demográfico 2022: primeiros resultados [Internet]. Rio de Janeiro: IBGE; 2023 [citado 14 jun. 2025]. Disponível em: https://censo2022.ibge.gov.br
13. Andrade MJD, Lima FM, Daibert EF, Oliveira Ad. Queimaduras no Triângulo Mineiro (Brasil): estudo epidemiológico de uma unidade de queimados. Rev Bras Queimaduras. 2016;15(02):97–103 Disponível em: https://www.rbqueimaduras.com.br/details/301/pt-BR/queimaduras-no-triangulo-mineiro–brasil—estudo-epidemiologico-de-uma-unidade-de-queimados
14. Church D, Elsayed S, Reid O, Winston B, Lindsay R. Burn wound infections. Clin Microbiol Rev 2006;19(02):403–434. Doi: 10.1128/CMR.19.2.403-434.2006
15. Bessa D, Ribeiro A, Barros S, Silva C, Costa M. Perfil epidemiológico dos pacientes queimados no Hospital Regional de Urgência e Emergência de Campina Grande – Paraíba – Brasil. Rev Bras Ciênc Saúde. 2009;10(01):73–80
16. Graner M, Gutierre M, Salgado LS, et al. Who gets burned in Brazil? J Burn Care Res 2023;45(04):926–931. Doi: 10.1093/jbcr/irad062
17. Weber EU, Blais A-R, Betz NE. A domain-specific risk-attitude scale: measuring risk perceptions and risk behaviors. J Behav Decis Making 2002;15(04):263–290. Doi: 10.1002/bdm.414
18. Toolaroud PB, Attarchi M, Haghdoust RA, et al. Epidemiology of work-related burn injuries: A ten-year retrospective study of 429 patients at a referral burn centre in the north of Iran. Int Wound J 2023;20(09):3599–3605. Doi: 10.1111/iwj.14238
19. Stewart S, Juang D, Aguayo P. Pediatric burn review. Semin Pediatr Surg 2022;31(05):151217. Doi: 10.1016/j.sempedsurg.2022.151217
20. Peden M, Oyegbite K, Ozanne-Smith J, et al., editors. Burns. In: ______. World Report on Child Injury Prevention. Geneva: World Health Organization; 2008. Disponível em: https://www.ncbi.nlm.nih.gov/books/NBK310640/
21. Abreu JRPd, Oliveira JFPd. Racismo no Brasil: negacionismo e suas consequências. Psicanálise (Porto Alegre) 2021;23(01):150–165. Doi: 10.60106/rsbppa.v23i1.780
22. Bagheri T, Fatemi MJ, Saberi M, Rahbar A, Momeni M. The Effect of Education on Primary School Students’ Knowledge Regarding Burn Prevention Measures and Actions to Take. J Burn Care Res 2021;42(02):220–227. Doi: 10.1093/jbcr/iraa138
23. Snelling S, Challoner T, Lewis D. Burns and socioeconomic depri-vation: the experience of an adult burns centre. Burns 2021;47 (08):1890–1895. Doi: 10.1016/j.burns.2021.02.019
24. Neves JBO, Ferreira MO, Santos TM. Perfil epidemiológico dos pacientes internados na unidade de queimados de um hospital de ensino de Minas Gerais. Rev Bras Cir Plást 2022;37 (01):26–32
25. Chen J, Wang Y. Characteristics and risk factors for electrical burn injuries: a study based on World Health Organization Global Burn Registry. Burns 2024;50(05):1116–1121. Doi: 10.1016/j.burns.2024.01.014
26. Pinto ACS, Costa KLN, Almeida Filho PP, Oliveira Júnior JL, Rocha MNS. Avaliação do perfil epidemiológico de pacientes adultos queimados internados em um centro de referência no interior do estado da Bahia, Brasil. Rev Bras Cir Plást 2022;37(01):66–70. Doi: 10.5935/2177-1235.2022RBCP0011
27. Longo S, Legramante JM, Rizza S, Federici M. Vasovagal syncope: An overview of pathophysiological mechanisms. Eur J Intern Med 2023;112:6–14. Doi: 10.1016/j.ejim.2023.03.025
28. Kiley JL, Greenhalgh DG. Infections in Burn Patients. Surg Clin North Am 2023;103(03):427–437. Doi: 10.1016/j.suc.2023.02.005
29. Orbay H, Ziembicki JA, Yassin M, Egro FM. Prevention and Management of Wound Infections in Burn Patients. Clin Plast Surg 2024;51(02):255–265. Doi: 10.1016/j.cps.2023.11.003
30. Kiley JL, Greenhalgh DG. Infections in Burn Patients. Surg Clin North Am 2023;103(03):427–437
1. Medicine Program, Universidade Federal do Rio Grande do Norte, Natal, RN, Brazil
2. Burn Treatment Center, Hospital Monsenhor Walfredo Gurgel (HMWG), Natal, RN, Brazil
3. Department of Infectious Diseases, Universidade Federal do Rio Grande do Norte,
Natal, RN, Brazil
4. Department of Surgery, Universidade Federal do Rio Grande do Norte, Natal, RN,
Brazil
Data Availability
Financial Support The authors declare that they did not receive financial support from agencies in the public, private or non-profit sectors to conduct the present study.
Address for correspondence Bárbara Xavier Gomes da Silva, Curso de Medicina, Universidade Federal do Rio Grande do Norte, Avenida Nilo Peçanha 620, Petrópolis, Natal, RN, 59012-300, BraZil (e-mail: babixavier26@gmail.com).
Article received: June 15, 2025.
Article accepted: November 24, 2025.
Conflict of Interests The authors have no conflict of interests to declare.
Editor-in-Chief: Dov Charles Goldenberg.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket