



Original Article - Year 2026 - Volume 41Issue 1
High-Definition Liposuction Assisted by a Third-Generation Ultrasound Device: Retrospective Analysis of Postoperative Outcomes
Lipoaspiração de alta-definição assistida por dispositivo ultrassônico de terceira geração: Análise retrospectiva de desfechos pós-operatórios

ABSTRACT
Introduction High-definition liposuction underwent a significant evolution with ultrasound emulsification technologies, which were introduced two decades ago and are continuously refined.
Objective To retrospectively evaluate the postoperative outcomes in patients undergoing high-definition liposuction using the Sound Amplification of Frequency Energy at Resonance (SAFER, FAGA Medical) technology, with emphasis on the surgical technique and safety aspects of the procedure. All surgeries were performed at Centro Hospitalar Santa Mônica in the municipality of Erechim, state of Rio Grande do Sul, Brazil.
Methods The current descriptive and retrospective study included 88 patients who underwent surgery between July 2023 and June 2024. The data collected included operative time, blood loss length of hospital stay, and the incidence of complications (seroma, burns etc.).
Results Efficient adipose tissue emulsification and improved three-dimensional body contour definition were observed. The mean operative time was of 286±20 minutes, the mean blood loss was of 300±80 mL, and the mean hospital stay was of 24±6 hours. The overall complication rate was of 6.8%, with no serious adverse events.
Conclusion High-definition liposuction assisted by a third-generation ultrasound aspiration device appears to be a safe and effective technique to enhance superficial anatomical definition, with outcomes comparable to those reported in the contemporary medical literature.
Keywords: plastic surgery procedures; postoperative care; lipectomy; body contouring; patient safety
RESUMO
Introdução A lipoaspiração de alta-definição tem se beneficiado de tecnologias de emulsão ultrassônica, desenvolvidas há cerca de duas décadas e continuamente aprimoradas.
Objetivo Descrever retrospectivamente os desfechos pós-operatórios de pacientes submetidos à lipoaspiração de alta-definição com tecnologia Sound Amplification of Frequency Energy at Resonance (SAFER, (FAGA Medical), com ênfase na técnica e nos aspectos de segurança associados ao procedimento. As cirurgias foram realizadas no Centro Hospitalar Santa Mônica, em Erechim, Rio Grande do Sul.
Métodos Trata-se de um estudo descritivo e retrospectivo de 88 pacientes operados entre julho de 2023 e junho de 2024. Foram coletados dados de tempo operatório, perda sanguínea, período de internação e incidência de complicações (seroma, queimaduras etc.).
Resultados Observou-se emulsificação eficiente do tecido adiposo e delineamento tridimensional do contorno corporal, com tempo cirúrgicomédio de 286±20 minutos, perda sanguínea média de 300±80mL e internação média de 24±6 horas. A taxa global de complicações foi de 6,8%, sem eventos adversos graves.
Conclusão A lipoaspiração de alta-definição com aparato de aspiração ultrassônica de terceira geração demonstrou-se aparentemente segura e eficaz para revelar tridimensionalmente a anatomia superficial de relevo, com estatísticas compatíveis com as da literatura médica contemporânea.
Palavras-chave: procedimentos de cirurgia plástica; cuidados pós-operatórios; lipectomia; contorno corporal; segurança do paciente
Introduction
Liposuction has undergone continuous evolution since its introduction, eventually becoming a consolidated and systematically-employed surgical technique.1 Superficial liposuction has historically been associated with risks such as contour irregularities and tissue necrosis. The advent of third-generation devices, such as the Sound Amplification of Frequency Energy at Resonance (SAFER, FAGA Medical) device, has enabled greater precision in adipose tissue emulsification, reducing tissue trauma and enabling aspiration over broader anatomical areas.2 Lipo-suction was initially described by Illouz in 1983,3 who highlighted its effectiveness in promoting skin retraction and refining esthetic contours. In Brazil, Avelar4 made significant contributions to the understanding of subcuta-neous tissue anatomy and its implications for the selection and indication of liposuction, emphasizing the importance of an anatomical approach to ensure procedur-al safety.
More recently, Garcia et al.5 reported advances in third-generation ultrasound-assisted liposuction, focusing on es-thetic contouring of the posterior trunk and gluteal regions. Hoyos and Millard2 further expanded this concept by intro-ducing dynamic three-dimensional ultrasound-assisted as-piration. The conceptual basis of the three-dimensional approach remains grounded in these studies.
High-definition liposuction surgery requires navigation between the compartments of adipose tissue. This three-dimensional approach contrasts with the traditional technique, which advocates manipulation restricted to the deep (lamellar) layer.6
Introduced in 2001, the Vibration Amplification of Sound Energy at Resonance (VASER, Solta Medical) system repre-sents the third generation of ultrasonic liposuction devices. Its development was based on the discovery that a frequency of 36.6 Hz induces resonance in adipocytes. The device can also deliver acoustic energy in pulsatile or continuous modes, enabling its adaptation to the histological character-istics of superficial tissues, thereby reducing procedural risks.7
The SAFER device, manufactured in Brazil, was introduced just over 1 year ago. It incorporates the physical properties of third-generation ultrasonic devices already established in several scientific studies. The efficiency of this device is attributed to a sound frequency of 36.6 Hz, which induces adipocyte resonance through cavitation, enabling the adipo-cytes to detach without damaging the surrounding tissues8 (►Fig. 1).


In the present study, no imaging studies were performed to confirm complete emulsification of the lamellar layer. Instead, the intraoperative assessment relied on ultrasound imaging to visualize the adipose tissue layers. Postoperative safety was evaluated using standardized clinical criteria, including pain, edema, hematoma formation, and local tem-perature changes. The routine use of hyperbaric oxygen therapy sessions during the first three postoperative days may represent a potential source of bias, as it could mask possible complications by accelerating tissue healing and reducing inflammation.
Objective
The current study aimed to retrospectively evaluate the postoperative complications and the safety profile of high-definition liposuction performed with ultrasonic-assisted retraction technology (SAFER) at Centro Hospitalar Santa Mônica, in the municipality of Erechim, state of Rio Grande do Sul, Brazil, between July 2023 and June 2024.
Methods
The present is a retrospective study based on a review of medical records. All patients included signed an informed consent form. The study was conducted in accordance with the principles of the Declaration of Helsinki and Resolution no. 466/2012 of the Brazilian National Health Council. The institutional Ethics in Research Committee approved the study under protocol number CAAE 81613124.1.0000.5351.
Inclusion and Exclusion Criteria
Eligible patients included men and women aged ::: 18 years who presented with localized subcutaneous fat deposits and underwent third-generation ultrasound-assisted high-definition liposuction using the SAFER device. The exclusion criteria were patients with severe diseases and/or limiting clinical comorbidities; women within the first year post-partum, pregnant, or breastfeeding, patients with body dysmorphic disorder, those with inflammatory or infec-tious skin conditions in areas adjacent to the surgical site, and overweight or obese subjects (body mass index [BMI] > 29 kg/m2).
Preoperative Assessment
Preoperative assessment included laboratory and comple-mentary tests according to age group, followed by a prean-esthetic evaluation conducted by the anesthesiology team.
SAFER
The SAFER device consists of an integrated system compris-ing an ultrasonic console, a handpiece, atraumatic titanium cannulas, skin ports, and foot pedals (►Fig. 2).


Skin Ports
Skin ports are used at surgical-access sites to provide thermal protection from ultrasonic vibrations. They are routinely inserted in the intergluteal cleft, anterior and posterior axillary lines, pubic region, umbilical scar, and inframam-mary folds (►Fig. 3).


Handpiece
The handpiece conducts ultrasonic energy and is directly connected to the ultrasonic console, with fittings for inter-changeable probes. As a safety measure, the surgeon attaches the titanium cannula to the handpiece.
A threaded locking mechanism secures the probe with 180° of rotation, ensuring proper coupling (►Fig. 4). Energy dispersion is then tested in saline solution to prevent tissue damage.


Probes
Probe insertion (►Fig. 5) into the surgicalaccess sites follows the standard technique used in conventional lipo-suction, consisting of gentle back-and-forth movements without the application of force. The procedure may begin in the areolar layer when strategically planned, followed by progression to the lamellar layer.


The system includes probes of varying diameters, with grooves near the tip to enhance energy transmission to emulsify the adipose tissue.7 Fewer rings at the tip are associated with greater precision and energy delivery. Dif-ferent designs are available to optimize treatment across anatomical regions.
Preoperative Marking
The physical examination includes a detailed analysis of adipose tissue distribution across several body regions, documenting abdominal and truncal fat thickness, as well as muscle mass.
Marking is performed with the patient in the standing position, beginning with areas planned for complete removal of the lamellar layer of the subcutaneous tissue.
Key abdominal landmarks include the linea alba, costal margin, lateral borders of the rectus abdominis, anterior superior iliac spines, and inguinal ligaments. In this region, three-dimensional transition zones lie along the semilunar line and the external oblique muscles, particularly in their caudal depressions.
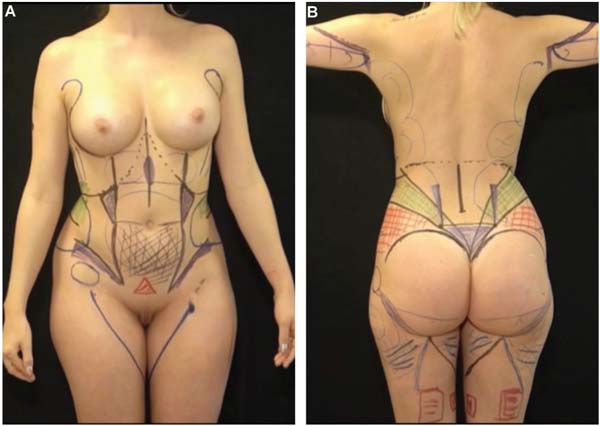
Equally important, relevant posterolateral landmarks in-clude the superior borders of the gluteus maximus muscles, the posteroinferior iliac spines, the erector spinae muscles, and the transition between the upper and lower back, following the topography of the lumbosacral fascia, where the point of greatest body convexity lies. A line is drawn from the anterosuperior iliac spine, and another, from the point of greatest inflection of the female curvature-corresponding to the eleventh rib-extending to the intergluteal cleft. This approach results in the formation of two triangles, one superior, and the other, inferior (shown in green and red, respectively, in ►Figs. 6A,B).





Operative Technique
Patient preparation in the operating room begins with the induction of general anesthesia, according to the protocol.
Subsequently, an indwelling urinary catheter is placed, along with compression stockings, intermittent pneumatic compres-sion devices, and active warming. As a fundamental principle to use the ultrasonic device, the procedure is performed in three stages: infiltration, emulsification, and aspiration.
Positioning
The procedure begins with the patient in the prone position, enabling wide exposure of the anatomical regions. Upon completion of this stage, the patient is placed in the supine position.
In both positions, strategic access ports are created in concealed areas: 1) back - intergluteal cleft and posterior axillary fold; 2) abdomen - pubic region, umbilical scar, inframammary folds, and anterior axillary region. Following infiltration, these access sites are fitted with skin ports to facilitate probe movement and prevent adjacent thermal injury.
Infiltration
The super-wet infiltration technique is used for both super-ficial and deep layers of the skin. A power-assisted liposuc-tion device with a 3-mm basket cannula is used for fluid infiltration.
The routine infiltrate-to-aspirate ratio is 2:1, using a solution of warmed saline, epinephrine, ropivacaine, and tranexamic acid (1 vial of epinephrine per 500 mL of saline plus 5 mL of 7.5% ropivacaine and 1 vial of tranexamic acid). Infiltration is performed before skin-port insertion. Main-taining adequate hydration of the subcutaneous tissue dur-ing the emulsification phase is essential, as the emulsion protects the epidermis from the ultrasonic energy dissipated by the device.8
Emulsification
Probe insertion follows the standard back-and-forth excur-sion movement used in traditional liposuction, without applying force, maintaining the probe parallel to the tissue during complete emulsification of the areolar layer. For optimal energy delivery to the lamellar layer, the probe is introduced at an approximately 45° angle relative to the planned treatment area.
As a general principle, emulsification begins in the superficial (areolar) layer and progresses to the deeper (lamellar) layer. According to SAFER recommendations, emulsification should be performed for approximately 2 minutes per 100 mL of infiltrate solution, or until tissue resistance is no longer perceived.
In denser tissues, such as in secondary or tertiary surgeries, a 1-ring probe is used with device power up to 80% in continuous mode, because energy dispersion is concentrated at the distal tip of the probe under these circumstances.
In the axial skeleton, two-ring probes are recommended, using pulsed mode in superficial layers and continuous mode in deeper layers, with power settings of approximately 70 and 80% respectively. Three-ring probes, which provide greater lateral energy dispersion, are suitable for more delicate tissues, such as those found in the extremities. In these cases, the device is typically set to 60% of power in pulsed mode (►Table 1). In our practice, the emulsification phase lasts approximately 30 to 40 minutes per patient position.
| Site | Probe | Mode | Frequency |
|---|---|---|---|
| Upper and lower limbs | 3.7 mm (3 rings) | Pulsatile | 60-70% |
| Abdomen/Back | 3.7 mm (2 rings) | Continuous/Pulsatile | 70-80% |
| Fibrous tissue | 3.7 mm (1 ring) | Continuous | 80% |

Liposuction
Liposuction begins with the selection of an appropriate cannula diameter according to the characteristics of the treatment area. The technique recommends initiating aspi-ration in the lamellar layer and completing it in the superfi-cial (areolar) layer.
Lamellar Layer
Fat aspiration follows the conventional tissue-removal tech-nique, using a fan-shaped pattern with the surgeon’s palm guiding the movement, enabling tactile feedback of the cannula, positioned at approximately 45°, while avoiding traumatic endpoints. The cannulas are Mercedes-type with three ports and diameters of 3 and 4 mm.
Areolar Layer
Superficial liposuction is strategically performed over the borders of muscle groups, including the linea alba, inguinal ligament, and lateral border of the rectus abdominis muscle, using delicate, precise, and controlled movements to allow visualization of the main three-dimensional anatomical land-marks of the superficial contour.
Smaller-diameter cannulas are essential for this layer; our practice uses 3.0-mm cannulas, maintaining the instrument parallel to the skin surface to avoid injury to the subdermal plexus.
Transition (Negative Spaces)
In these regions, the goal is to delicately blend the interfaces between different anatomical units (muscle groups and adjacent anatomical contours) through gradual and progres-sively-decreasing aspiration, moving from shadowed areas toward light-reflecting regions. This approach enables the visualization of a smooth skin tonal transition, correspond-ing to a gradual increase in tissue thickness from shadowed to highlighted areas. Cannulas with a 3.0-mm diameter are preferred in these regions.
Closed-suction drains are placed after liposuction is com-plete. Our practice uses Blake (Ethicon, Inc.) drains in the suprapubic region and PortoVac® (Braile Biomédica, São José do Rio Preto, SP, Brasil) drains in the lumbosacral region. The drains are maintained for approximately 7 days and/or until output is lower than 50 mL per 24 hours.
Postoperative Management
The patients are fitted with compressive garments, and intermittent pneumatic compression devices are initiated intraoperatively and maintained throughout hospitalization. Thye garments are applied by the multidisciplinary team at the end of the procedure and reassessed after 4 hours to ensure proper positioning and preservation of vasculariza-tion in thin flaps.
On the first postoperative day, the patients begin manual lymphatic drainage, performed daily at the institution for a minimum of 10 days. In addition, 3 sessions (performed on postoperative days 1, 2, and 3.8) of hyperbaric oxygen therapy are administered to reduce edema and promote tissue healing, as previously described.7
Venous thromboembolism prophylaxis includes the use of elastic compression stockings extending to the proximal third of the lower limbs, intermittent pneumatic compression during the intraand postoperative periods, early ambulation, and low-molecular-weight heparin for 21 days.
The patients are followed postoperatively by a multidis-ciplinary team from postoperative days 1 to 10, with additional follow-up visits at days 15, 30, 60, 90, and 180. Immediate results are often affected by edema and the early stages of wound healing during the first 3 to 4 weeks, with progressive improvement thereafter. Areas of fibrosis may develop between 4 and 8 weeks, with a tendency toward spontaneous resolution by the fourth post-operative month.
Results
In the current retrospective study, based on an analysis of medical records, we evaluated postoperative surgical com-plications in patients undergoing high-definition liposuction using SAFER, correlating the findings with those of the existing literature (►Table 2).
| Perioperative complications (0-48 hours | Immediate postoperative complications (1-7 days) | Late postoperative complications (1 week-3 months) |
|---|---|---|
| Necrosis | Cellulitis | Seroma |
| Injury caused by cannula/port/endpoint | Paresthesia/Transient or permanent sensorial abnormality | Prolonged edema |
| Anesthetic complications | Hyperpigmentation/Hypopigmentation | Fibrosis |

A total of 88 patients were included; the sample was predominantly female, with 80 patients (90.9%), while the 8 male patients accounted for 9.1% of the cases.
Complications were assessed by the attending surgeon and a multidisciplinary team during standardized clinical follow-up visits. No cases of infection, skin irregularities, or clinically-significant asymmetries were observed at the 30-and 60-day follow-ups. The mean estimated blood loss was 300 ± 80 mL per patient.
The age of the female patients ranged from 18 to 55 (mean: 36) years. In the male group, the mean age was 38 (range: 32-54) years. The overall mean BMI was 24.51 kg/m2. The mean operative time was 286 (range: 241-433) minutes.
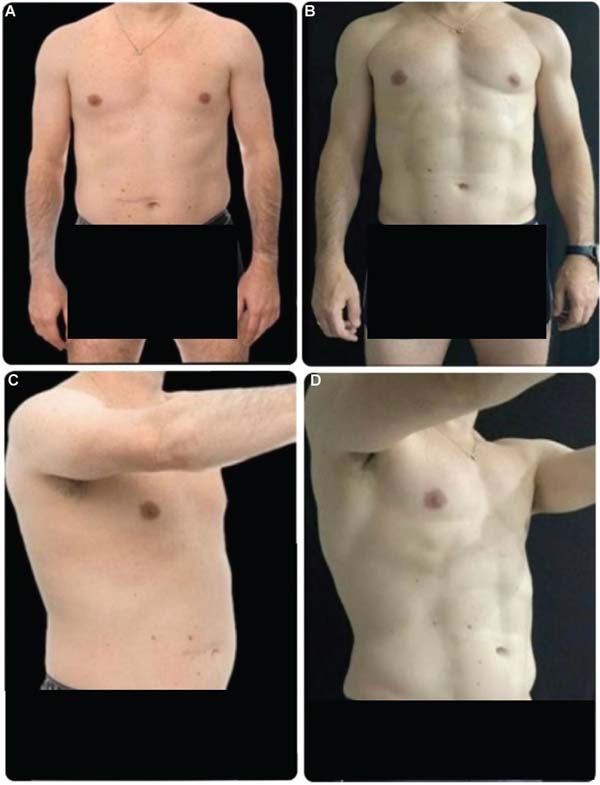
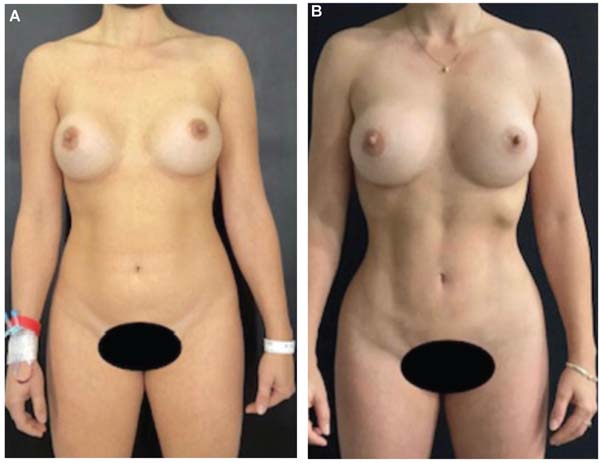
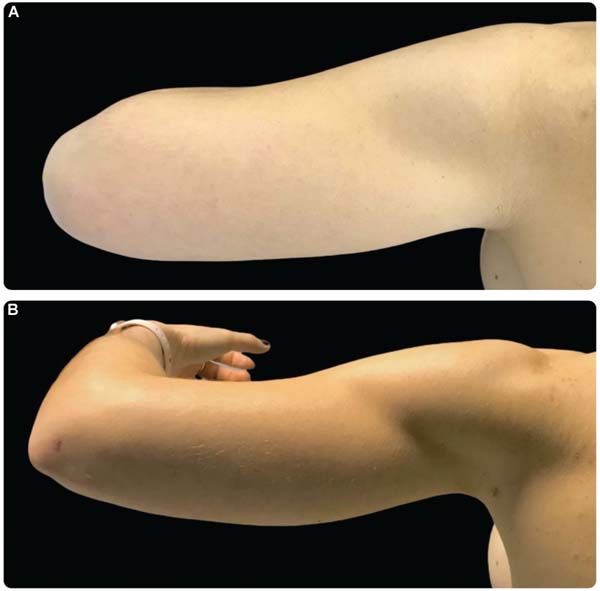
In our series, there was 1 case of skin burn (at the skin-port site in the anterior axillary region), attributed to a damaged device component, and 5 cases of seroma, resulting in an overall postoperative complication rate of 6.8%. There were no major complications (►Table 3). These findings are supported by the postoperative results (►Figs. 6-10).
| Complications | Patients (n) | % |
|---|---|---|
| Prolonged edema | 0 | 0 |
| Thermal injury at the insertion site | 1 | 1.1 |
| Hyperpigmentation | 0 | 0 |
| Epidermal injury | 0 | 0 |
| Seroma | 5 | 5.7 |
| Fibrosis | 0 | 0 |
| Sensorial abnormality | 0 | 0 |
| Anesthetic complications | 0 | 0 |
| Total | 6 | 6.8 |


Discussion
In the present study, 88 patients underwent ultrasound-assisted liposuction using SAFER for the treatment of lip-odystrophy. The findings suggest that subcutaneous tissue emulsification using pulsed and continuous ultrasound modes is effective and safe.9
The aspirated material contained a mean of 91% superna-tant fat. Blood loss was minimal, since the infranatant aspirated fraction was small, and no clinical measures were required to correct depletion in any case.
In the present series, the seroma rate was 5.7%, despite the routine use of drains. This incidence is higher than that reported in the literature. A review published in The Ameri-can Journal of Cosmetic Surgery in 2023 reported a mean seroma rate of 2.3% in mediumand large-volume liposuction procedures without ultrasound technology.10 This difference may be related to the three-dimensional approach and the simultaneous manipulation of the areolar and lamellar layers, which may increase the risk of seroma formation.
The aspirated material was analyzed using a sedimenta-tion/decantation method in a graduated cylinder for 30 minutes, according to the protocol described by Garcia and Nathan,11 to estimate the percentage of supernatant fat. The mean value observed was 91% (range: 80-95%), indicat-ing high efficiency of the ultrasonic emulsification.
These findings are consistent with those reported by Garcia Junior and Nathan,11 who demonstrated that third-generation ultrasonic devices reduce blood loss by approxi-mately 6.5-fold compared with other techniques.
In a literature review with statistical analysis of surgical complications related to liposuction, Jewell et al.8 reported an overall complication rate of 13.5%, which is higher than that observed in our series.
A comprehensive review of postoperative complications in liposuction by Dixit and Wagh12 reported a rate of 18.7% of cutaneous hyperpigmentation, attributed to manipula-tion of the areolar layer and subsequent injury to the subdermal plexus. The low incidence of complications in superficial liposuction with the use of third-generation ultrasound is an important issue when we compare the rates found, for, in these surgeries, we strategically manip-ulate, in 100% of the cases,, the areolar layer with adipose emulsification and subsequent liposuction, to enable the three-dimensional body contouring approach. It is impor-tant to emphasize the minute amount of adverse events in this specific context, since in our sample the outcomes were completely opposite from those found in the aforemen-tioned literature.
In a multicenter, prospective, randomized study, Nagy and Vanek reported a 53% greater degree of skin retraction with VASER compared with traditional liposuction in contralater-al anatomical regions of the same patient.
In our series, all procedures were performed using SAFER, and clinically relevant skin laxity was not observed during follow-up. Considering that ultrasound-assisted emulsification relies on similar physical principles of energy dispersion and adipose tissue interaction, this finding may be associated with the tissue retraction effect described in the literature. In our practice, based on experience with third-genera-tion ultrasound technology since 2012, additional skin-tightening devices have often not been required. Although subtle, the tissue retraction promoted by third-generation devices appears to be effective across multiple anatomical regions, supporting the findings by Nagy e Vanek.13
Based on these principles-namely, tissue retraction and safe manipulation of the areolar layer without tissue devi-talization-it is possible to approach the adipose tissue in a controlled manner to reveal its three-dimensional geome-try.7,14 We highlight that the harmony of the outcome is a reflection of the grade tridimensionality to be revealed in all anatomical units with similar intensity, and, it is important to emphasize, while maintaining consistency with the patient’s lifestyle (►Fig. 11).


Hoyos and Millard2 reported that firstand second-gener-ation ultrasonic devices were associated with severe burns and necrosis due to uncontrolled superficial energy disper-sion. These complications have been largely mitigated with the advent of third-generation technology,11,15,16 which has enabled the safe application of more superficial lipoplasty techniques. Our findings also support this concept.
Techniques aimed at enhancing anatomical definition increase surgical complexity. Therefore, strict adherence to safety principles, standardization of strategies for each anatom-ical region according to its histological and geometric character-istics, and the adoption of diligent rules throughout the learning curve are essential to achieve consistent outcomes.
It is worth noting that all procedures analyzed in the current study consisted exclusively of liposuction, with no association with concomitant surgeries. In our technique, complete removal of the lamellar layer of the subcutaneous tissue is pursued in the areas defined during preoperative marking,17 although no imaging method is used for objective confirmation. Assessment is based on intraoperative inspec-tion, palpation, and real-time ultrasonography. The routine use of hyperbaric oxygen therapy during the first three postoperative days aims to enhance tissue regeneration and mitigate inflammatory responses. This practice was imple-mented systematically only in cases using SAFER technology and was not part of previous protocols for conventional liposuction performed by the team. Therefore, it represents an adjunctive, non-mandatory strategy which, in our experi-ence, may contribute to improved early healing outcomes.
Conclusion
The existing literature and our findings suggest that the use of SAFER, as applied in the technique described in the current retrospective study, is associated with low complication rates and effective body-contouring outcomes, aligning with established safety parameters.
However, although promising, these results should be interpreted with caution, given the slightly-higher compli-cation rate if one considers those reported by studies com-paring the technique herein described with conventional techniques. Further standardization and well-designed ran-domized controlled trials are necessary to better define the safety profile and consolidate the evidence supporting this approach.
References
1. Jewell M. Ultrasonic-Assisted Liposuction: Introduction and His-toric Perspectives. In:Garcia O Jr., editor. Ultrasound-Assisted Liposuction: Current Concepts and Techniques [Internet]. Cham, Switzerland: Springer; 2020:3-8 [cited May 7, 2025]. . Doi: 10.1007/978-3-030-26875-6_1
2. Hoyos AE, Millard JA. VASER-assisted high-definition liposculp-ture. Aesthet Surg J 2007;27(06):594-604. Doi: 10.1016/j.asj.2007.08.007
3. Illouz YG. Illouz’s technique of body contouring by lipolysis. Clin Plast Surg 1984;11(03):409-417
4. Avelar JM. Principles of Liposuction. In:Illouz YG, Sterodimas A, editors. Adipose Stem Cells and Regenerative Medicine [Internet]. Berlin/Heidelberg: Springer; 2011:19-29 [cited May 7, 2025]. . Doi: 10.1007/978-3-642-20012-0_3
5. Garcia O, Pena PSC, Pazmino P. Suction-Assisted Lipectomy and Brazilian Butt Lift. In:Thaller SR, Panthaki ZJ, editors. Tips and Tricks in Plastic Surgery [Internet]. Cham, Switzerland: Springer; 2022:151-189 [cited May 7, 2025]. . Doi: 10.1007/978-3-030-78028-9_10
6. Gomes RS, Nicolau GV. Abdominal liposuction: evolving from high to medium definition. Rev Bras Cir Plást 2021;36(02): 134-143. Doi: 10.5935/2177-1235.2021RBCP0059
7. Friedman T, Menashe S, Landau G, et al. Hyperbaric Oxygen Preconditioning Can Reduce Postabdominoplasty Complications: A Retrospective Cohort Study. Plast Reconstr Surg Glob Open 2019;7(10):e2417. Doi: 10.1097/GOX.0000000000002417
8. Jewell ML, Fodor PB, Pinto EBdS, Al Shammari MA. Clinical application of VASER-assisted lipoplasty: a pilot clinical study. Aesthet Surg J 2002;22(02):131-146. Doi: 10.1067/ maj.2002.123377
9. Stein MJ, Matarasso A. High-Definition Liposuction in Men. Clin Plast Surg 2022;49(02):307-312. Doi: 10.1016/j.cps.2022.01.003
10. Troell RJ. Lipoabdominoplasty: Comparing Ultrasound-Assisted and Power-Assisted Techniques. Am J Cosmet Surg 2023;40(04): 279-292. Doi: 10.1177/07488068221099153
11. Garcia O Jr, Nathan N. Comparative analysis of blood loss in suction-assisted lipoplasty and third-generation internal ultra-sound-assisted lipoplasty. Aesthet Surg J 2008;28(04):430-435. Doi: 10.1016/j.asj.2008.04.002
12. Dixit VV, Wagh MS. Unfavourable outcomes of liposuction and their management. Indian J Plast Surg 2013;46(02):377-392. Doi: 10.4103/0970-0358.118617
13. Nagy MW, Vanek PFA Jr. A multicenter, prospective, randomized, single-blind, controlled clinical trial comparing VASER-assisted Lipoplasty and suction-assisted Lipoplasty. Plast Reconstr Surg 2012;129(04):681e-689e. Doi: 10.1097/PRS.0b013e3182442274
14. Grolleau JL, Rouge D, Chavoin JP, Costagliola M. [Severe cutaneous necrosis after ultrasound lipolysis. Medicolegal aspects and re-view]. Ann Chir Plast Esthet 1997;42(01):31-36
15. Scheflan M, Tazi H. Ultrasonically assisted body contouring. Aesthet Surg Quarterly 1996;16(02):117-122. Doi: 10.1016/ S1090-820X(96)70034-1
16. Seidel W, Garcia CP. Use of VaserTM plus liposuction in body contouring surgery. Rev Bras Cir Plást 2020;35(02):161-167. Doi: 10.5935/2177-1235.2020RBCP0028
17. Almeida ARHD, Mafra AVC, Araújo GKMD. Metodologia para análise de resultados em lipoaspiração. Rev Bras Cir Plást 2011; 26(02):288-292 Available from: https://www.rbcp.org.br/Content/imagebank/pdf/v26n2a16.pdf
1. Advanced Center for Plastic Surgery, Centro Hospitalar Santa Mônica, Erechim, RS,
Brazil
2. Instituto Dr. José Frota, Fortaleza, CE, Brazil
Address for correspondence Felipe Massignan, Núcleo Avançado em Cirurgia Plástica, Centro Hospitalar Santa Mônica, Erechim, RS, Brazil (e-mail: nucleoavancadocirurgiaplastica@gmail.com).
Artigo submetido: 27/06/2024.
Artigo aceito: 14/12/2025.
Editor-in-Chief: Dov Charles Goldenberg.
Conflict of Interests
The authors have no conflict of interests to declare.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket