



Case Reports - Year 2011 - Volume 26 -
Intergluteal sulcus reconstruction: a case report
Reconstrução do sulco interglúteo: relato de caso
ABSTRACT
Introduction: The concept of female beauty has changed over time, but the shape and projection of the glutei have always been symbols of femininity. The buttocks have received increasing media attention in recent years, resulting in an increase in the demand for gluteal surgery. Objective: The purpose of this case report is to demonstrate the surgical correction of a deformity of the intergluteal sulcus, with preservation of the sacrocutaneous ligament. Case Report: A female patient complaining of a deformity of the intergluteal sulcus and hypoplastic glutei underwent surgical treatment consisting of reconstruction of the intergluteal sulcus with preservation of the sacrocutaneous ligament, implantation of a silicone gluteal prosthesis in the intramuscular plane, and hip liposuction. Conclusion: The understanding of the principles of the XYZ technique, and particularly of the anatomy of the sacrocutaneous ligament, allowed for correction of the intergluteal sulcus deformity and remodeling of the posterior contour.
Keywords: Buttocks/surgery. Prostheses and implants. Reconstructive Surgical Procedures/methods.
RESUMO
Introdução: O conceito de beleza feminina tem mudado ao longo dos anos, porém a forma e a projeção das nádegas permanecem como símbolos de máxima feminilidade. A exposição corporal, especialmente da região glútea, tem proporcionado aumento da procura pela cirurgia de gluteoplastia. Objetivo: O propósito deste relato é demonstrar a correção cirúrgica de uma deformidade do sulco interglúteo, utilizando a preservação do ligamento sacrocutâneo. Relato do Caso: Paciente do sexo feminino, com queixa de deformidade do sulco interglúteo e nádegas hipoplásicas. O tratamento cirúrgico consistiu na reconstrução do sulco interglúteo por meio de preservação do ligamento sacrocutâneo, implantação de prótese de silicone glútea no plano intramuscular e lipoaspiração das ancas. Conclusão: O entendimento dos princípios da técnica XYZ, em particular do ligamento sacrocutâneo, possibilitou a correção da deformidade do sulco interglúteo e o remodelamento do contorno posterior da paciente.
Palavras-chave: Nádegas/cirurgia. Próteses e implantes. Procedimentos Cirúrgicos Reconstrutivos/métodos.
The buttocks have received increasing media attention in recent years, resulting in an increase in the demand for gluteoplasty, a surgical procedure that can significantly improve the posterior contour of the buttocks; further, the recent advances in gluteoplasty techniques have also made this a popular procedure1.
In 1894, Morestin described the support system for the soft tissue structures of the gluteal region2. This system is composed of dense connective tissue that forms connections between the bone ligament structure on the back of the pelvis, the dermis supporting the skin, and the subcutaneous tissue of the gluteal region. The intergluteal sulcus is formed by these strong ligamentous connections between the deep layer of the dermis and the sacrococcyx.
A century later, Gonzalez described the sacrocutaneous ligament3. This anatomical structure is a simple expansion of the sacral ligaments (part of Morestin's2 intergluteal crease suspension system), and has been termed the sacrocutaneous ligament because of its extreme tensile strength and abundance of dense connective tissue3-5.
Our objective is to demonstrate the importance of preserving the sacrocutaneous ligament when repairing a congenital deformity of the intergluteal sulcus.
CASE REPORT
A 25-year-old woman (weight, 57 kg; height, 1.62 m; hip circumference, 97 cm) presented with hypoplastic buttocks, a deformity of the intergluteal sulcus, and minor fat deposition at the hips. The patient had no history of receiving injections in the intergluteal sulcus or of infection or trauma in that area, and reported that the deformity had been present since birth (Figure 1). On physical examination, a deviation of the intergluteal sulcus to the right side, with a lack of depth in the third upper region, was diagnosed.

Figure 1 - Preoperative: congenital deformity at the intergluteal sulcus.
Surgery consisted of retraction of the sacrocutaneous ligament3 (Figure 2); release of a small retraction of the lateral sacrocutaneous ligament on the left side (Figure 3); placement of two smooth, round, 330-ml implants on the intramuscular plane using the XYZ technique4,5; and hip liposuction.

Figure 2 - Intraoperative: preservation of the sacrocutaneous ligament. Note the released retraction on the left side of the intergluteal sulcus below the Gilles hook.
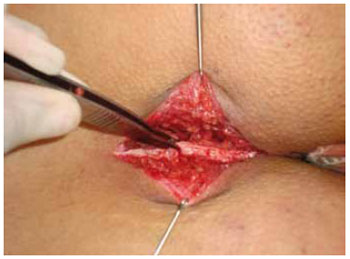
Figure 3 - De-epidermized sacrocutaneous ligament.
The patient recovered well postoperatively and was pleased with the outcome of the surgery (Figures 4 to 6).

Figure 4 - Immediately after the operation: reconstruction of the intergluteal sulcus and implantation of the intramuscular gluteal prosthesis.

Figure 5 - A: Preoperative. B: Three months postoperatively.
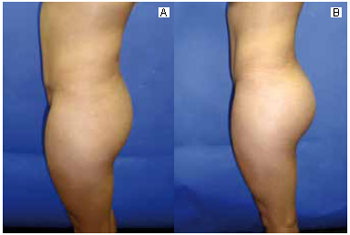
Figure 6 - A: Preoperative. B: Three months postoperatively.
DISCUSSION
The concept of female beauty has changed with time, but the shape and projection of the glutei have always been considered symbols of femininity1. Over the past 40 years, many plastic surgeons have developed techniques and tactics to provide patients with a more sensual silhouette in the gluteal region1,3-10.
In this report, we showed the importance of physical examination of the posterior contour of the patient, which allowed for correction of the congenital deformity of the intergluteal sulcus, liposuction of the hip region, and remodeling of the buttocks by placing silicone implants intramuscularly, in accordance with the principles of the XYZ technique described by Gonzalez4,5.
This technique establishes clear anatomic landmarks to guide the ideal plane of detachment within the gluteus maximus. The detachment is not limited by the upper limit of the pyramidal muscle, thereby allowing for placement of implants at a lower position. The sacrocutaneous ligament is preserved, and the aponeurotic linking system between the skin and deep tissues is maintained4,5,8,9.
Some surgical techniques for the introduction of a silicone prosthesis in submuscular6, intramuscular7 or subfascial8 areas, through an incision directly over the intergluteal sulcus and dissection of the subcutaneous tissue, may destroy the anatomy of the intergluteal sulcus.
The preservation of the sacrocutaneous ligament is achieved by performing a fusiform incision, leaving an island of skin that contains in its depth the sacral ligament expansions forming the intergluteal sulcus. This provides many advantages, such as allowing reconstruction of the intergluteal sulcus in cases of congenital or acquired deformity, serving as a reference for the normal depth of the sulcus, providing anchorage to adjacent structures at the intergluteal incision, separating the detachment between the buttocks, controlling postoperative infection or formation of seromas, optimizing second-intention healing in the case of dehiscence, and ensuring long-term maintenance of the intergluteal fold as the entire anatomy of the region is preserved3-5.
CONCLUSION
Preservation of the sacrocutaneous ligament is important for maintaining the anatomy of the intergluteal sulcus, allowing for safe reconstruction.
REFERENCES
1. Mendieta CG. Classification system for gluteal evaluation. Clin Plast Surg. 2006;33(3):333-46.
2. Morestin H. l`appareil suspenseur dupli inter-fessier in these. Paris:Bibliotéque Faculte Medicine;1894.
3. Gonzalez R. Prótese para região glútea. In: Tournieux AAB, ed. Atualização em cirurgia plástica estética. São Paulo:Robe;1994. p.557-61.
4. Gonzalez R. Augmentation gluteoplasty: the XYZ method. Aesthetic Plast Surg. 2004;28(6):417-25.
5. Gonzalez R. Buttocks reshaping: posterior contour surgery. A step-by-step approach. Rio de Janeiro:Indexa;2006.
6. Robles JM, Tagliapietra JL, Grandi MA. Gluteoplastia de aumento: implante submuscular. Cir Plast Iberolatinoam. 1984;X:4-9.
7. Vergara R, Marcos M. Intramuscular gluteal implants. Aesthetic Plast Surg. 1996;20(3):259-62.
8. De la Penã JA, Rubio OV, Cano JP, Cedillo MC, Garcés MT. Subfascial gluteal augmentation. Clin Plast Surg. 2006;33(3):455-22.
9. Almeida Júnior GL, Almeida EG. Implante glúteo - técnica XYZ: estudo retrospectivo. Rev Bras Cir Plást. 2008;23(2):103-11.
10. Almeida Júnior GL, Castro WC, Almeida EG. Implante glúteo e posição intramuscular parcial: relato de caso. Rev Bras Cir Plást. 2009;24(2):242-5.
Plastic Surgeon, Member of the Brazilian Society of Plastic Surgery, Brasília, DF, Brazil.
Corresponding author:
Genes Lopes de Almeida Junior
QS 01 Rua 210 lote 40 - Centro Empresarial - Taguatinga Shopping - Torre B, sala 728
Brasília, DF, Brazil CEP 71950-904
E-mail: geneslopes@terra.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Received: July 23, 2009
Accepted: September 17, 2009
Work performed at the author's private clinic, Brasília, DF, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket