



Case Reports - Year 2011 - Volume 26 -
Lower extremity burns with bone exposure: reconstruction with the dermal regeneration template
Queimadura com exposição óssea dos membros inferiores: reconstrução com matriz de regeneração dérmica
ABSTRACT
Introduction: The standard treatment for lower extremity burns with exposed bone is vascularized tissue transfer; however, this option is often unavailable or is technically difficult. The dermal regeneration template, a bioengineered skin substitute, is a remarkable alternative to the traditional reconstructive choices. Case Report: This report describes two cases of burns involving the lower extremities of patients admitted to the São José Hospital Burns Unit between January 2007 and December 2008 that were treated with dermal regeneration templates. Both patients had bilateral deep burn injuries with exposed bone affecting the anterior surface of the lower legs and were treated with tangential excision of the burn eschar and dermal regeneration template placement. Four weeks later, after the template engraftment, the thin outer layer of silicone was removed and epidermal coverage was restored with a split thin skin graft. Stable wound coverage was achieved and no further surgical procedures were required to maintain wound closure. Conclusion: The use of the dermal replacement template expands the reconstructive options for complex burn (and nonburn) wounds, prevents the need for prolonged staged procedures, allows successful coverage of vital structures without the use of a flap and, particularly, ensures extremity preservation.
Keywords: Burns. Lower extremity. Reconstruction. Leg/surgery.
RESUMO
Introdução: As soluções reconstrutivas das queimaduras dos membros inferiores com exposição óssea (transferência de tecidos vascularizados) e dos defeitos do escalpe, não susceptíveis de encerramento com retalhos locais (expansão tecidual), são complexas, morosas e, por vezes, inviáveis. O recurso a substitutos cutâneos biológicos, como a matriz de regeneração dérmica, constitui uma importante alternativa às soluções reconstrutivas tradicionais. Relato dos casos: Estudo retrospectivo de 246 doentes com queimaduras dos membros inferiores, admitidos na Unidade de Queimados/Serviço de Cirurgia Plástica do nosso Centro Hospitalar, entre janeiro de 2007 e dezembro de 2008. Os autores apresentam 2 casos clínicos com queimaduras bilaterais das pernas e com exposição óssea. Nos dois casos, realizou-se desbridamento tangencial e encerramento das áreas cruentas com um substituto cutâneo, a matriz de regeneração dérmica. Na 4ª semana após a aplicação da matriz, o componente externo da membrana bilaminar foi substituído por enxerto de pele parcial. Obteve-se cobertura estável das áreas cruentas, sem necessidade de procedimentos cirúrgicos adicionais. Conclusões: A utilização de substitutos dérmicos expande as opções reconstrutivas nos casos de queimaduras com exposição óssea dos membros inferiores. A utilização da matriz biológica permitiu a preservação dos membros nos dois pacientes. A matriz de regeneração dérmica possibilitou uma cobertura estável de estruturas vitais, sem necessidade de transferência ou expansão tecidual e com morbilidade mínima.
Palavras-chave: Queimaduras. Extremidade inferior. Reconstrução. Pernas/cirurgia.
Treatment of extensive and deep burns of the lower extremities, especially in critical regions such as the anterior leg, remains a major challenge for the plastic surgeon1,2. The amputation risk of an extremity after a burn injury increases from 1.5% to 18-40% in the case of circumferential or fourth-degree burns3,4. Deep burns in the leg that result in exposed bone and tendon are not eligible for coverage with a skin graft and require multiphase and complex therapeutic strategies involving different levels of pyramid reconstruction. The use of several muscular5 and myocutaneous flaps (sometimes neurovascular)6 has been described with varying degrees of success. Reconstructions with free and pedicled flaps usually involve highly complex technical procedures, with considerable failure rates (12%) and the risk of amputation (18%)3,7, which are related to the patient's condition (instability, hemodynamic imbalance), the small percentage of surrounding viable tissue, and rarity of receptor areas for transfer.
The dermal regeneration template (Integra), a biosynthetic dermal substitute created in 1981 by Burke and Yanas and approved by the US Food and Drug Administration in 1996, was initially developed for the treatment of burns (primary coverage of third-degree burns after early debridement)8,9. Currently, it is widely used in various areas of reconstructive surgery2,8-10. It comprises a bilaminar xenogeneic system: the deeper plate, equivalent to the dermal layer, corresponds to a template composed of bovine collagen and glycosaminoglycans (chondroitin-6-sulfate) derived from shark cartilage, and the epidermal component is represented by a thin silicone layer designed to simulate the physiological skin barrier, controlling water loss and preventing infection. The material, which serves as a template for fibroblastic and endothelial cell development and migration, becomes vascularized in 2-4 weeks while undergoing a concomitant remodeling process that turns it into dermal tissue. In this phase, the silicone layer is removed and safely replaced with a partial skin graft1.
Although the scientific literature largely supports the use of this biosynthetic template in burned areas9-13, studies of this dermal substitute in the treatment of severe burns with exposed bone are lacking. Unlike skin grafts, which depend on immediate inoculation and soaking to maintain viability, the biosynthetic template is an acellular structure and therefore does not require immediate vascularization. The neovascularization occurring in 2-4 weeks enables low-vascularized vital structures (tendon, bone) to receive stable coverage without the morbidity of a flap transfer.
The aim of this paper is to present two cases of severe burns in the lower extremities with exposed bone and highlight the effectiveness of the dermal regeneration template for stable coverage of the defects with minimal associated morbidity.
CASE REPORT
The artificial skin substitute is composed of a porous template of collagen and chondroitin-6-sulfate coated with a thin layer of a polysiloxane polymer (silicone). Its architecture provides ideal physicochemical conditions and humidity, leading to dead space elimination, prevention of water loss, control of bacterial invasion, while simultaneously ensuring cell migration and vascular growth, which are responsible for neoderm formation.
This report describes two cases of lower extremity burns treated with dermal regeneration template application that were selected from 246 cases at the Burns Treatment Unit of the São José Hospital in Lisbon, Portugal, between January 2007 and December 2008. Both patients were male and presented with severe lower extremity burns of the anterior leg with bone exposure and extensive tissue destruction (Figures 1 and 2).

Figure 1 - Deep burns (third- and fourth-degree burns) in the lower extremities with tibial exposure. Anterior left knee joint coverage with internal twin muscle flaps and an autograft with partial skin in the meshwork (mesh graft, 1:3) was performed.
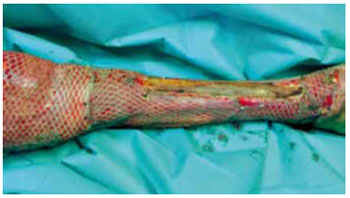
Figure 2 - Deep burns (third- and fourth-degree burns) in the lower extremities with tibial exposure. Open area coverage with an autograft comprising partial skin in the meshwork (mesh graft 1:3) was performed.
The surgical procedure was identical in both cases. Initially, early debridement of the burned area and coverage of the open area surrounding the exposed bone with a partial skin graft were performed. The older patient, aged 84, had an exposed anterior left knee joint, which was covered with internal twin muscle flaps.
Given the impossibility of closure of the exposed bone area by secondary intention, excisional debridement for obtaining bleeding edges and tangential ostectomy for necrotic bone tissue removal were considered. Multiple point (holes) ostectomies were performed in the anterior part of the tibias, devoid of periosteum, in patient 1. Open area coverage was performed with a dermal regeneration template cut according to the wound dimensions and fixed to the edge of the open area with staples. A moderately compressive dressing of gauze impregnated with paraffin and swabs soaked in saline was applied. The dressing was changed every two days. Upon verifying the neovascularization of the total dermal template (between 21 and 28 days), the silicone layer was replaced with a skin graft. After the first postgraft dressing (4 and 5 days), the wound was dressed with gauze impregnated with paraffin and pads soaked in 0.9% saline every two days.
Both patients were surgically treated twice, first for dermal regeneration template application to the unbridled and poorly vascularized bed and then to restore epidermal coverage through the silicone blade replacement with a partial skin graft. In both cases, stable defect coverage was ensured without the need for additional surgical procedures. Both patients regained their ambulatory status and had no complications, including infection.
Patient 1
An 84-year-old man was hospitalized after an accidental fire-related burn (fall in the fireplace). The total burned body surface area was approximately 20% and was limited to the lower extremities. He mostly had deep second-degree burns and 4% third- and fourth-degree burns involving the anterior left knee joint and anterior surface of both legs. After early debridement of the burned area, open area coverage of the anterior left knee with internal twin muscle flaps and the whole open area surrounding the exposed bone with partial skin grafts was performed (Figures 1 and 2). The exposed bone area was covered with a dermal regeneration template after debridement, osteotomies (holes), and tangential ostectomy (Figures 3 to 5). After the 28th day, the dermal template was completely vascularized (Figure 6) and the silicone layer was replaced with a thin partial skin graft (mesh graft, 1:3). Good healing was noticed, with full integration of the graft and stable coverage of the whole open area (Figures 7 to 9).

Figure 3 - Devitalized tissue debridement and ostectomy (tangential and perforating) of the anterior right tibia.

Figure 4 - Dermal regeneration template for exposed bone closure and fixation with staples.

Figure 5 - Dressing with gauze impregnated with paraffin and pads soaked in 0.9% saline.

Figure 6 - Fourth-week postapplication appearance of the dermal regeneration template over the right and left tibias, when the silicone layer was replaced with a thin partial skin autograft.

Figure 7 - Second week after the application of a thin partial skin autograft on the dermal regeneration template.

Figure 8 - Appearance of the right leg one month after the application of a thin partial skin autograft. The defect coverage ensures extremity preservation.

Figure 9 - Appearance of the left leg one month after the application of a thin partial skin autograft. The defect coverage ensures extremity preservation.
Patient 2
A 64-year-old man was hospitalized after an accidental fire-related burn (fire). The total burned body surface area was approximately 59%, mostly comprising deep second- and third-degree burns; the anterior surface of both legs had about 3% third- and fourth-degree burns (Figure 10). After excisional debridement of the burned area, bilateral exposure of the anterior tibia was identified. Tangential ostectomy and coverage of the area with a dermal regeneration template were performed (Figures 11 and 12). The open areas surrounding the exposed bone were closed with partial skin grafts. The dermal substitute integration enabled defect coverage (Figure 13). On the 21st day, the dermal template was completely vascularized (Figure 14) and the silicone layer was replaced with a thin partial skin graft (mesh graft, 1:3; Figure 15). Good healing was noticed, with full integration of the graft and stable coverage of the whole open area (Figure 16).

Figure 10 - Deep burns (fourth-degree burns) in the lower extremities with tibial exposure. The open area periphery was covered with a partial skin meshwork autograft (mesh graft, 1:3).

Figure 11 - One week after tangential debridement and application of a dermal regeneration template on the left tibia.

Figure 12 - Three weeks after the application of a dermal regeneration template on the left leg.

Figure 13 - Three weeks after the application of a dermal regeneration template on the left leg. The dermal substitute integration enables defect coverage.

Figure 14 - Three weeks after the application of a dermal regeneration template. The presence of a well-vascularized neoderm is verified, which is capable of withstanding a thin partial skin autograft.
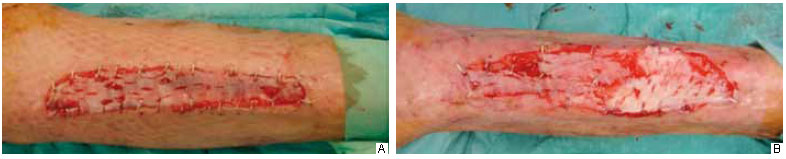
Figure 15 - Three weeks after the application of a dermal regeneration template. The silicone layer is replaced with a thin partial skin autograft.

Figure 16 - Two weeks after the application of a thin partial skin autograft. The defect coverage ensures extremity preservation.
DISCUSSION
Skin substitutes obtained from bioengineered tissues have considerably increased the number of reconstructive options in several areas such as traumatology, oncology, and chronic wound treatment, particularly for patients with burns8,14. The dermal regeneration template that has been used for nearly 30 years is proven to be of good quality and is widely used15-19.
The biosynthetic template is acellular and therefore "not viable" when applied; however, it is subsequently incorporated and vascularized by the surrounding tissue1,2,20. Given the absence of living cells in the template, there are no metabolic needs to fulfill, unlike in skin grafts, which depend entirely on the vascularity of the bed to which they are applied. On average, the biosynthetic template requires 21 days for vascularization; however, in greatly adverse situations (deep burns with severe tissue destruction), the process may be extended, without affecting the treatment success and outcome20.
The treatment of severe burns in the lower extremities with exposed bone invariably poses various problems in addition to the potential threat of amputation. In these cases, the skin graft does not resolve the open area coverage problem, because the wound bed (open area with exposed bone) does not ensure the necessary vascularization of the graft. Vascularized tissue transfer has revolutionized the treatment of these complex cases21,22; once bound to the transposed tissue, an entire vascular network is obtained, which is extremely important for healing. Whenever possible, this is the recommended reconstructive option. However, not all patients are candidates for transfer of vascularized tissues: patients with unstable hemodynamic changes secondary to severe trauma or burns, patients with extensive tissue injuries that make local tissue mobilization impossible, and those without receptor areas capable of support flap transfer. Jeng et al.2 showed a significant reduction in the amputation rate (31.5% in the control group vs. 5.7% in the study group) by using the dermal regeneration template for severe and deep burns. In this context, for more complex cases, the dermal regeneration template should be an effective and safe alternative, allowing defect closure without the risk of tissue loss due to necrosis.
Application of this dermal substitute requires a clean receptor bed, free of devitalized or necrotic tissue; a second surgery for the silicone-layer replacement with a skin graft; and dressing and monitoring by qualified personnel. The lengthy process prolongs patient recovery, compared with the use of autologous tissues (flaps), which emphasizes its status as "salvage therapy" and justifies its use in special cases, such as outcome refractory to the treatment or high risk of extremity loss. Further, the dermal regeneration template is very expensive, and therefore it is not widely used.
Lee et al.1 described an algorithm for using the dermal regeneration template in the treatment of burn patients. According to the authors, one of the following 4 criteria should be met: extensive burns with lack of viable skin to ensure burned area coverage with a 2:1 meshwork graft; extensive burns in children and lack of sufficient skin to ensure adequate open area coverage with skin grafts (given the greater importance of functional and esthetic recovery); deep burns on the face without the possibility to cover the burned area with full-thickness grafts; and exposure of important structures (tendon, bone, nerve) unsuited for graft-based coverage. The Department of Plastic and Reconstructive Surgery of the São José Hospital has no algorithm for using the dermal regeneration template and recently began therapy with the template; however, the case studies presented here confirm and reinforce the information previously considered by Lee et al.1.
CONCLUSION
The dermal regeneration template is assumed to be an effective and safe alternative for treating severe, deep burns in the lower extremities with exposed bone without the need for reconstructive autologous alternatives and amputation risk. This dermal substitute enables stable defect coverage of variable dimensions and is readily available. It causes minimal morbidity of the donor area and ensures a satisfactory aesthetic result.
REFERENCES
1. Lee LF, Porch JV, Spenler W, Garner WL. Integra in lower extremity reconstruction after burn injury. Plast Reconst Surg. 2008;121(4):1256-62.
2. Jeng JC, Fidler PE, Sokolich JC, Jaskille AD, Khan S, White PM, et al. Seven years' experience with Integra as a reconstructive tool. J Burn Care Res. 2007;28(1):120-6.
3. Parrett BM, Pomahac B, Demling RH, Orgill DP. Fourth-degree burns to the lower extremity with exposed tendon and bone: a ten-year experience. J Burn Care Res. 2006;27(1):34-9.
4. Li X, Liang D, Liu X. Compartment syndrome in burn patients. A report of five cases. Burns. 2002;28(8):787-9.
5. Klein HW, Reavi DW. Salvage of both lower extremities using simultaneous bilateral gastrocnemius and soleus muscle flaps: a case report. J Burn Care Rehabil. 1998;9(2):184-6.
6. Katsaros J, Proudman TW. The very long posterior tibial artery island flap. Br J Plast Surg. 1991;44(8):599-601.
7. Baumeister S, Köller M, Dragu A, Germann G, Sauerbier M. Principles of microvascular reconstruction in burn and electrical burn injuries. Burns. 2005;31(1):92-8.
8. Heimbach D, Luterman A, Burke J, Cram A, Herndon D, Hunt J, et al. Artificial dermis for major burns. A multi-center randomized clinical trial. Ann Surg. 1988;208(3):313-20.
9. Lorenz C, Petracic A, Hohl HP, Wessel L, Waag KL. Early wound closure and early reconstruction. Experience with a dermal substitute in a child with 60 per cent surface area burn. Burns. 1997;23(6):505-8.
10. Dantzer E, Queruel P, Salinier L, Palmier B, Quinot JF. Dermal regeneration template for deep hand burns: clinical utility for both early grafting and reconstructive surgery. Br J Plast Surg. 2003;56(8):764-74.
11. Frame JD, Still J, Lakhel-LeCoadou A, Carstens MH, Lorenz C, Orlet H, et al. Use of dermal regeneration template in contracture release procedures: a multicenter evaluation. Plast Reconst Surg. 2004;113(5):1330-8.
12. Klein MB, Engrav LH, Holmes JH, Friedrich JB, Costa BA, Honari S, et al. Management of facial burns with a colagen/glycosaminoglycan skin substitute-prospective experience with 12 consecutive patients with large, deep facial burns. Burns. 2005;31(3):257-61.
13. Ryan CM, Schoenfeld DA, Malloy M, Schulz JT 3rd, Sheridan RL, Tompkins RG. Use of Integra artificial skin is associated with decreased length of stay for severely injured adult burn survivors. J Burn Care Rehabil. 2002;23(5):311-7.
14. Burke JF, Yannas IV, Quinby WC Jr, Bondoc CC, Jung WK. Successful use of a physiologically acceptable artificial skin in the treatment of extensive burn injury. Ann Surg. 1981;194(4):413-28.
15. Moiemen NS, Vlachou E, Staiano JJ, Thawy Y, Frame JD. Reconstructive surgery with Integra dermal regeneration template: histologic study, clinical evaluation, and current practice. Plast Reconst Surg. 2006;117(7 Suppl):160S-174S.
16. Chou TD, Chen SL, Lee TW, Chen SG, Cheng TY, Lee CH, et al. Reconstruction of burn scar of the upper extremities with artificial skin. Plast Reconst Surg. 2001;108(2):378-84.
17. Suzuky S, Shin-ya K, Kawai K, Nishimura Y. Application of artificial dermis prior to full-thickness skin grafting for resurfacing the nose. Ann Plast Surg. 1999;43(4):439-42.
18. Abai B, Thayer D, Glat PM. The use of a dermal regeneration template (Integra) for acute resurfacing and reconstruction of defects created by excision of giant hairy nevi. Plast Reconst Surg. 2004;114(1):162-8.
19. Komorowska-Timek E, Gabriel A, Bennett DC, Miles D, Garberoglio C, Cheng C, et al. Artificial dermis as an alternative for coverage of complex scalp defects following excision of malignant tumors. Plast Reconst Surg. 2005;115(4):1010-7.
20. Yannas IV. Studies on the biological activity of the dermal regeneration template. Wound Repair Regen. 1998;6(6):518-23.
21. Afifi AM, Mahboub TA, Losee JE, Smith DM, Khalil HH. The reverse sural flap: modifications to improve efficacy in foot and ankle reconstruction. Ann Plast Surg. 2000;61(4):430-6.
22. Wang XC, Lu Q, Li XF, Burd A, Zhao BC, Wang YY, et al. Reversed anterolateral thigh adipofascial flap for knee and proximal calf defects. Burns. 2008;34(6):868-72.
1. Practitioner Resident of the Plastic and Reconstructive Surgery and Burns Unit of the Centro Hospitalar de Lisboa (Hospital de São José), Portugal.
2. Member of the Portuguese Society of Plastic and Reconstructive Surgery; Member of the Portuguese Society of Burns. Preceptor and Graduate Hospital Assistant of the Plastic and Reconstructive Surgery and Burns Unit of the Centro Hospitalar de Lisboa (Hospital de São José), Portugal.
3. Member of the Brazilian Society of Plastic Surgery; Member of the Ibero-Latin American Federation of Plastic Surgery; Specialist Member of the College of Reconstructive Plastic and Aesthetic Surgery by the Medical Council of Portugal; Member of the Portuguese Society of Burns. Member of the Portuguese Society of Plastic and Reconstructive Surgery; Preceptor and Hospital Assistant of the Plastic and Reconstructive Surgery and Burns Unit of the Centro Hospitalar de Lisboa (Hospital de São José), Portugal.
Corresponding author:
Ana Cristina Pereira Cardoso da Silva Guerra
Rua Mateus Vicente, 15, 9º D.
Lisboa, Portugal - CP 1500-445
E-mail: anacristinacardososilva@gmail.com
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Received: November 26, 2009
Accepted: February 4, 2010
Work performed at the Serviço de Cirurgia Plástica e Reconstrutiva e Unidade de Tratamento de Queimados do Centro Hospitalar de Lisboa Central (Hospital de São José) - (Department of Plastic and Reconstructive Surgery and Burns Treatment Unit of the Centro Hospitalar de Lisboa - Hospital de São José), Lisbon, Portugal.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket