



Original Article - Year 2013 - Volume 28 -
Fat grafting in breast reconstruction
Lipoenxertia em reconstrução mamária
ABSTRACT
BACKGROUND: Breast reconstruction often requires a second surgical procedure to correct visible irregularities of the breast contour. Lipofilling (fat grafting) consists of a surgical technique that improves or corrects such deformities, and serves as an alternative to other conventional techniques that have higher morbidity rates and complexity. In the present study, we aimed to describe our 8-year experience with a fat grafting method for correcting contour deformities of breasts that were previously reconstructed using conventional techniques.
METHODS: All patients in this study previously underwent mastectomy (total or partial) and some degree of breast reconstruction. The fat was obtained by liposuction using a syringe, and was gently rinsed with a saline solution in a stainless steel sieve, poured into a 60 cc syringe, and grafted after a few minutes.
RESULTS: In total, 112 patients underwent surgery between 2005 and 2012. There was one (8.9%) case of total loss of the fat graft, while 22 (19.6%) patients had small palpable nodules. The average graft volume was 100 cc, and multiple procedures were required to achieve the desired volume.
CONCLUSIONS: Fat grafting is a safe technique with low morbidity rates that demonstrates high surgeon and patient satisfaction levels, despite the need for multiple procedures to achieve good results.
Keywords: Transplants. Adipose tissue. Mammaplasty. Breast neoplasms.
RESUMO
INTRODUÇÃO: Frequentemente, a reconstrução mamária requer um segundo tempo cirúrgico para corrigir visíveis irregularidades no contorno da mama. A lipoenxertia constitui-se em uma técnica cirúrgica que pode melhorar ou corrigir essas deformidades em substituição a outras técnicas convencionais de maior morbidade ou complexidade. O objetivo deste estudo é demonstrar um método de correção de defeitos de contorno de mamas reconstruídas previamente pelas técnicas convencionais com enxerto de gordura, após 8 anos de experiência.
MÉTODO: Todas as pacientes incluídas neste estudo foram previamente submetidas a mastectomia (total ou parcial) e a algum tipo de reconstrução mamária. A gordura foi obtida por meio de método clássico de lipoaspiração com seringa, delicadamente lavada com solução salina em uma peneira de aço inoxidável, decantada em uma seringa de 60 cc e enxertada após alguns minutos.
RESULTADOS: Foram operadas 112 pacientes no período de 2005 a 2012. Houve 1 (8,9%) caso de perda total do enxerto de gordura, 22 (19,6%) pacientes apresentaram pequenos nódulos palpáveis, o volume médio enxertado foi de 100 cc e foram necessários múltiplos procedimentos para se alcançar o volume desejado.
CONCLUSÕES: A lipoenxertia constitui-se em uma técnica segura, com baixa morbidade e altos índices de satisfação do cirurgião e das pacientes, apesar de necessitar de múltiplos procedimentos cirúrgicos para atingir bom resultado.
Palavras-chave: Transplantes. Tecido adiposo. Mamoplastia. Neoplasias da mama.
Autologous adipose tissue has been used to correct soft tissue abnormalities since the beginning of the last century. Its soft and natural texture, availability in sufficient quantities, and potentially permanent integration are all characteristics that make adipose tissue the ideal physiological filling material.
In the mid-1980s, the popularity of liposuction using a syringe increased, which enabled the collection of fat in a in a simple and safe manner and increased surgeon interest in the free fat transfer method1. However, three issues remained to be clarified: first, the fear that fat necrosis could be mistaken for cancerous calcification2; second, the degree to which the injected adipose tissue was reabsorbed was unpredictable; and third, an unclear risk of potential cancer recurrence was noted, which required close observation.
In 2005, Spear et al.3 reported that autologous fat transplantation was a very safe technique that could significantly improve or correct contour deformities following breast reconstruction that would otherwise require additional procedures with greater complexity and higher risks; however, this procedure of lipofilling required repeated injections to achieve the desired result.
In the present study, we aimed to indicate our 8-year experience with a fat grafting method for correcting the contour deformities of breasts previously reconstructed using conventional techniques.
METHODS
A total of 112 patients who underwent lipofilling following breast reconstruction at a philanthropic hospital (Instituto do Câncer do Ceara) and a private clinic (Artclinic) were included in the current study. Patients' data were collected from medical records (from the outpatient ward and clinic) and recorded in a form specifically created for this study.
Surgical Technique
The procedural steps were as follows:
With the patient in a standing position, the areas of liposuction and lipofilling were marked (Figure 1).
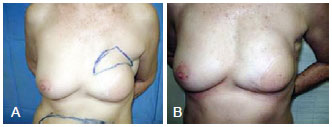
Figure 1 - In A, preoperative appearance with marking of the area to be grafted in the upper pole of the left breast (frontal view). In B, appearance 1 year following 70 cc lipofilling (frontal view).
2. In the operating room, sedation was administered intravenously, followed by regional anesthesia in the donor area (abdomen) and local anesthesia in the receiving area (breast).
3. A small-gauge cannula was used to inject a 0.9% saline solution with epinephrine, diluted to 1:500,000. After a few minutes, a 60 cc syringe attached to a blunt 4 mm cannula was inserted via a small incision using a No. 15 blade in the selected area (abdomen) that would receive the liposuction.
4. The fat was obtained using the standard syringe method1.2.
5. The obtained adipose tissue was placed into a sterile steel sieve to separate the solid (fat) and liquid (oil, saline solution, saline) components through gravity (Figure 2).

Figure 2 - Separation by gravity of the adipose tissue obtained from liposuction using a steel sieve.
6. The fat was decanted into a 60 cc syringe and held vertically (Figure 3).
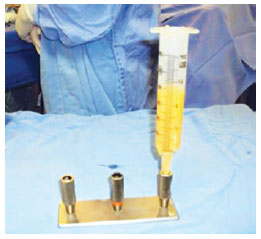
Figure 3 - Decanting of the fat into a 60 cc syringe, held vertically.
7. Thereafter, the decanted fat was transferred into 10 ml or 20 ml syringes (Figure 4).
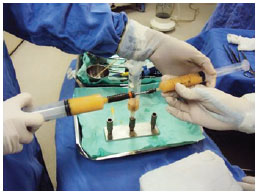
Figure 4 - Transfer of the decanted fat to smaller syringes.
8. Blunt 2 mm liposuction cannulae were used to establish tunnels that allowed for fractionated re-injection via several passages, in the subcutaneous tissue of the depressions to be corrected around the breast, through a single 5 mm incision (Figure 5).

Figure 5 - Re-injection of the fat into the deformities.
The patients were discharged on the first postoperative day and prescribed oral antibiotics (cephalosporin) and non-steroidal anti-inflammatory drugs. They were instructed to avoid compression of the grafted breast and the use of dressings or a bra. The patients were followed up on the 7th day, 14th day, 1st month, 3rd month, and 6th month after surgery, when subsequent surgical procedures were performed, and when deemed necessary.
RESULTS
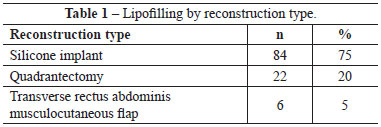
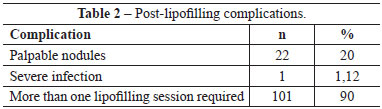
One hundred and twelve breasts were operated on by the same author over 8 years. Eighty-four (75%) patients had received silicone prostheses following mastectomy, while 22 (20%) had previously undergone quadrantectomies. The remaining patients received transverse rectus abdominis musculocutaneous flaps (Table 1).
More than one procedure was required in 101 (90%) of the patients. There was only 1 (1.12%) case of total loss of the fat graft (180 cc) in the second surgical procedure due to local infection. Twenty-two (20%) patients had small palpable nodules, without local effects (Table 2). The average volume of the transplanted fat was 100 cc (range, 40-300 cc).
The mean follow-up was 9 months after the last fat grafting session. The patient satisfaction rate was high, and each breast that underwent lipofilling had a soft and natural look. Figures 6 to 13 illustrate some cases of this series.

Figure 6 - In A and B, preoperative appearance of the markings in the area to be grafted in the upper pole of the left breast (frontal and left oblique views). In C and D, appearance 6 months after 100 cc lipofilling and replacement of the papillary-areolar complex (frontal and left oblique views).

Figure 7 - In A, preoperative appearance of the markings of the area to be grafted in the upper pole of the left breast (frontal view). In B and C, appearance 6 months after 100 cc lipofilling (frontal and left profile views).

Figure 8 - In A, B, and C, preoperative appearance (right oblique, frontal, and close-in right oblique views). In D, E, and F, appearance 6 months after 100 cc lipofilling (frontal, left oblique, and right oblique views).

Figure 9 - In A, preoperative appearance of the markings in the area to be grafted in the left breast (left oblique view). In B and C, appearance 4 months after a 60 cc lipofilling procedure (frontal and left oblique views).

Figure 10 - In A and B, left preoperative appearance (left oblique and left profile views). In C and D, appearance 6 months after two consecutive 120 cc lipofilling procedures (left oblique and left profile views).
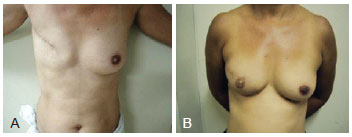
Figure 11 - In A, preoperative appearance (frontal view). In B, appearance 9 months after three consecutive 140 cc lipofilling procedures (frontal view).
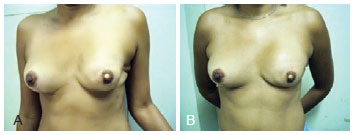
Figure 12 - In A, preoperative appearance (frontal view). In B, appearance 18 months after two consecutive 120 cc lipofilling procedures (frontal view).

Figure 13 - In A and B, preoperative appearance of markings on the right breast (frontal view). In C and D, appearance 14 months after 3 consecutive 120 cc lipofilling procedures (frontal view).
DISCUSSION
Despite the improvements in the various methods of primary breast reconstruction over the past 30 years and limitations in terms of the outcome following adjuvant radiotherapy, contour deformities persist in reconstructed breasts, which makes it difficult to achieve a desired natural look4.
There is currently a preference for silicone implants in primary breast reconstructions worldwide. Implants and autologous flaps utilized in the breast reconstructions often have areas of irregular contour that may affect any part of the breast, especially the upper pole - an area that is difficult to fix when a fine skin flap is left after mastectomy5. In addition, although quadrantectomies require a reconstruction method with aesthetic results, the use of radiotherapy and would also require immediate reconstruction, which may be associated with an increased failure rate, need for secondary reconstruction using more complex procedures, and/or elevated risk compared to traditional techniques. Fat injection, which can improve these areas in the majority of patients, yields good results and low morbidity rates. However, the key to successful fat transplantation involves mainly technical features (surgeon dependent) and depends on several factors during the three main phases: removal (collecting), purification, and replacement (injection)6-8.
We still collect the adipose tissue with a syringe, minimize its exposure to air, do not use any type of centrifugation system, and use small amounts of saline solution to clean the obtained fat, since we believe that growth factors, angiogenic properties, and other components of the primitive cells can be lost if the collected fat is thoroughly cleaned3,8-11. Although centrifugation of fat is a popular and effective method of purification, some studies have failed to demonstrate a significant increase in the survival of fat grafts purified in this manner8.
The case of total loss of a fat graft (180 cc) in the second half of the session due to infection was attributed to the fact that the patient was a smoker and had a history of previously reconstructed and irradiated breasts and an earlier loss of a prosthesis to infection.
Measuring fat reabsorption is difficult since the use of more reliable radiological methods such as computed tomography and nuclear magnetic resonance in the pre- and postoperative periods in all patients is financially unfeasible in Brazil. Thus, these evaluations were subjectively performed using physical examination (palpation) and digital images (photos) despite their known limitations12,13.
Three issues remain to be clarified. First, there was initial concern about the presence of fat necrosis that could be mistaken for cancerous calcifications. In recent years, advanced radiologic screening techniques have made it easier for radiologists to distinguish between alterations associated with benign necrosis of the breast tissue and those present in cancer10. The knowledge of the appearance of the breast from the perspective of mammography and ultrasound along with the evolution of fat necrosis patterns in patients who have undergone breast fat injection is required in post-lipofilling evaluations, and this knowledge from other patients who underwent normal breast procedures such as breast reduction or augmentation surgeries would also be useful.
Second, the degree to which the injected adipose tissue was reabsorbed is unpredictable. It is estimated that 30-40% of the volume is lost following the first surgical procedure. However, the reabsorption rate of secondary procedures is 20-30% lower2,9.
Third, the effect of such procedures on potential cancer recurrence is unknown. Adipocytes, preadipocytes, and progenitor cells may stimulate angiogenesis and cell growth. The tumor-stromal interaction can potentially induce the reappearance of cancer by "feeding" dormant breast cancer cells within the tumor bed. However, there is a lack of translational research that proves this concern from the clinical perspective, and no study of the effects of lipotransfer in human cells of in vivo breast cancer is currently available14,15.
It is noteworthy that the injection of adipocytes alone will not result in tumor recurrence. A vascular stroma supports the fat, and mesenchymal stem cells within the blood vessels and the pericytes around them are responsible for producing fat cells. It is also relevant to point out that the stromal vascular fraction, which has been used in wound treatment and breast reconstruction, contains stem cells, but the volume required for this method to be effective is unknown16.
CONCLUSIONS
Autologous fat grafting is an important option for correcting contour deformities that manifest in a previously reconstructed breast. It constitutes a simple, safe, inexpensive, and effective treatment with low morbidity rates and allows for the creation of new subcutaneous tissue accompanied by improved quality of the reconstructed breast skin, despite the disadvantageous feature that several sessions are needed to achieve the desired aesthetic results.
REFERENCES
1. Toledo LS, Mauad R. Fat injection: a 20-year revision. Clin Plast Surg. 2006;33(1):47-53.
2. Illouz YG, Sterodimas A. Autologous fat transplantation to the breast: a personal technique with 25 years of experience. Aesthetic Plast Surg. 2009;33(5):706-15.
3. Spear SL, Wilson HB, Lockwood MD. Fat injection to correct contour deformities in the reconstructed breast. Plast Reconstr Surg. 2005;116(5):1300-5.
4. Pestana IA, Campbell DC, Bharti G, Thompson JT. Factors affecting complications in radiated breast reconstruction. Ann Plast Surg. 2013;70(5):542-5.
5. Pereira LH, Sterodimas A. Aesthetic restoration of axillary contour deformity after lymph node dissection. J Plast Reconstr Aesthet Surg. 2008;61(2):231-2.
6. Gutowski KA; ASPS Fat Graft Task Force. Current applications and safety of autologous fat grafts: a report of the ASPS Fat Graft Task Force. Plast Reconstr Surg. 2009;124(1):272-80.
7. Rosing JH, Wong G, Wong MS, Sahar D, Stevenson TR, Pu LL. Autologous fat grafting for primary breast augmentation: a systematic review. Aesthetic Plast Surg. 2011;35(5):882-90.
8. Kanchwala SK, Glatt BS, Conant EF, Bucky LP. Autologous fat grafting to the reconstructed breast: the management of acquired contour deformities. Plast Reconstr Surg. 2009;124(2):409-18.
9. Panettiere P, Marchetti L, Accorsi D. The serial free fat transfer in irradiated prosthetic breast reconstructions. Aesthetic Plast Surg. 2009;33(5):695-700.
10. Pallua N, Pulsfort AK, Suschek C, Wolter TP. Content of the growth factors bFGF, IGF-1, VEGF, and PDGF-BB in freshly harvested lipoaspirate after centrifugation and incubation. Plast Reconstr Surg. 2009;123(3):826-33.
11. Delay E, Garson S, Tousson G, Sinna R. Fat injection to the breast: technique, results, and indications based on 880 procedures over 10 years. Aesthet Surg J. 2009;29(5):360-76.
12. Gosset J, Guerin N, Toussoun G, Delaporte T, Delay E. Radiological evaluation after lipomodelling for correction of breast conservative treatment sequelae. Ann Chir Plast Esthet. 2008;53(2):178-89.
13. Amara O, Bruant-Rodier C, Lehmann S, Bollecker V, Wilk A. Fat tissue transplant: restoration of the mammary volume after conservative treatment of breast cancers, clinical and radiological considerations. Ann Chir Plast Esthet. 2008;53(2):169-77.
14. Lohsiriwat V, Curigliano G, Rietjens M, Goldhirsch A, Petit JY. Autologous fat transplantation in patients with breast cancer: "silencing" or "fueling" cancer recurrence? Breast. 2011;20(4):351-7.
15. Rigotti G, Marchi A, Galiè M, Baroni G, Benati D, Krampera M, et al. Clinical treatment of radiotherapy tissue damage by lipoaspirate transplant: a healing process mediated by adipose-derived adult stem cells. Plast Reconstr Surg. 2007;119(5):1409-22.
16. Stocchero IN, Stocchero GF. Isolation of stem cells from human adipose tissue: technique, problems, and pearls. In: Illouz Y-G, Sterodimas A, eds. Adipose stem cells and regenerative medicine. Heidelberg: Springer-Verlag Berlin; 2011. p. 13-8.
1. Plastic surgeon, full member of the Sociedade Brasileira de Cirurgia Plástica (Brazilian Society of Plastic Surgery - SBCP), head of the Department of Plastic Surgery of the Instituto do Câncer do Ceará (Cancer Institute of Ceará), Fortaleza, CE, Brazil
2. Plastic surgeon, full member of the SBCP, tutor of the Plastic Surgery Service of the Hospital Geral de Fortaleza (General Hospital of Fortaleza), Fortaleza, CE, Brazil
3. Resident physician in the Department of Plastic Surgery of the Instituto Dr. José Frota (Dr. José Frota Institute), aspiring member of the SBCP, Fortaleza, CE, Brazil
Correspondence to:
Francisco José Fontenele Bezerra
Rua Barão de Aracati, 444 - ap. 900 - Meireles
Fortaleza, CE, Brazil - CEP 60115-080
E-mail: fco.fontenele@yahoo.com.br
Submitted to SGP (Sistema de Gestão de Publicações/Manager Publications System) of RBCP (Revista Brasileira de Cirurgia Plástica/Brazilian Journal of Plastic Surgery).
Article received: February 5, 2013
Article accepted: April 27, 2013
This study was performed at the Cancer Institute of Ceará and in the private clinic, Artclinic, Fortaleza, CE, Brazil.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket