



Reviw Article - Year 2014 - Volume 29 -
Augmentation gluteoplasty with intramuscular implants
Gluteoplastia de aumento com implantes intramusculares
ABSTRACT
INTRODUCTION: The buttocks are composed of muscles that control leg movement, with the gluteus maximus muscle playing an important role. In addition, as an erogenous zone, they are associated with sex-related function. Voluminous buttocks incite greater scrutiny and sexual desire, which has increased the demand for augmentation gluteoplasty with the use of silicone implants. Gluteal implants allow for effective reshaping and augmentation of the buttocks, in sharp contrast with the results obtained with other techniques. The implant pockets can be inserted in four different planes, namely the subcutaneous, subfascial, intramuscular, and submuscular planes. The ideal location of the gluteal implant is currently controversial, with arguments in favor of both the subfascial and intramuscular planes. The aims of this study were to introduce gluteoplasty techniques described in the literature that use the intramuscular plane as the implant insertion route and to determine the degree of patient satisfaction with results, as well the safety, applicability, and reproducibility of the technical procedures.
METHODS: This literature review is based on online electronic searches on the MEDLINE database in November 2011. The most frequently described immediate adverse effects of the technique include pain, wound dehiscence, seroma, and infection.
RESULTS: The patients were greatly satisfied. The XYZ procedure, which includes marking anatomical reference points to guide the intramuscular dissection, provides technical insight that ensures reproducible results and prevents complications such as palpable or perceptible implants.
CONCLUSION: This procedure has been demonstrated to produce natural and satisfactory results, with low complication rates.
Keywords: Intramuscular; Gluteus; Implants.
RESUMO
INTRODUÇÃO: As nádegas são constituídas por músculos responsáveis por movimentos das pernas, assumindo o músculo glúteo máximo o volume principal. Possuem uma função secundária, de cunho sexual, como zona erógena. O maior volume de nádegas desperta maior atenção e desejo sexual, o que tem levado a um aumento da procura pela cirurgia de gluteoplastia de aumento com utilização de implantes de silicone. Os implantes glúteos proporcionam uma remodelagem e aumento efetivo das nádegas que nem sempre são obtidos por outros métodos. Existem quatro planos para a colocação dos implantes glúteos: subcutâneo, subfascial, intramuscular e submuscular. Atualmente, há uma discussão sobre a posição ideal dos implantes glúteos, com defensores tanto do plano subfascial quanto intramuscular. O objetivo deste estudo foi apresentar as técnicas publicadas de gluetoplastia de aumento, que utilizam o plano intramuscular para acomodação dos implantes, e avaliar a satisfação com os resultados, assim como a segurança, a aplicabilidade e a reprodutibilidade dos procedimentos.
MÉTODOS: Este estudo constitui-se de uma revisão de literatura, elaborada através de uma pesquisa eletrônica de literatura, em novembro de 2011, através dos bancos de dados MEDLINE. As complicações imediatas mais frequentes são dor, deiscência da ferida, seroma e infecção.
RESULTADOS: Houve grande satisfação dos pacientes. A técnica XYZ, através da marcação de pontos de referências anatômicas para guiar a dissecção intramuscular no plano correto, permite uma compreensão necessária para reproduzi-las e evitar complicações como implantes visíveis e palpáveis.
CONCLUSÃO: Este procedimento tem se mostrado um método que produz resultados muito naturais e de longa duração, com baixas taxas de complicações.
Palavras-chave: Intramuscular; Glúteo; Implantes.
The buttocks are two fleshy, rounded structures posteriorly located in the pelvis and limited by an imaginary line that runs above the highest point of the iliac crests down to the infragluteal crease. The gluteus maximus muscle is responsible for most of the volume; but in the anterolateral region, the gluteus medius is superficially located and constitutes most of the volume of that region. The buttocks are also considered as an erogenous zone, which contributes to sex appeal.
Augmentation gluteoplasty can be performed by using autologous tissue obtained from the patient (fat, dermal fat flap, or muscle flap) or by using artificial materials (implants and fillings), either alone or in combination.
Gluteal implants effectively augment the buttocks area, producing a more desirable shape, which is not easy to achieve with other approaches. The desired round shape of the implant is achieved through a concentrated projection, which is not always the case with the fat flap.
The gluteal implants can be round or oval, filled with highly cohesive silicone or made of soft silicone blocks. Four approaches may be used for the insertion of the implant pockets, namely through the subcutaneous, subfascial, intramuscular, and submuscular planes.
In 1969, Bartels described augmentation gluteoplasty with subcutaneous implants. However, most of the reported results included delocalization, asymmetries, and capsular contractures1.
In 1984, Robles introduced a new augmentation technique with submuscular implants inserted through an incision in the midline sacral region2. Meanwhile, Vergara and Marcos3 published in 1996 a gluteal augmentation technique with the use of intramuscular implants. In 2000, De La Peña4 described the use of prostheses via the subfascial plane. Currently, the ideal placement of gluteal implants is controversial, with arguments in favor of both the subfascial and intramuscular planes. In countries where augmentation gluteoplasty has become popular, such as Brazil, the intramuscular plane has been preferred.
Gonzalez1 described the XYZ technique in 2004, establishing the procedures to be followed when performing the intramuscular detachment in the ideal plan, through marking of anatomical reference points to guide the dissection and prevent perceptible or palpable implants.
Surgical Procedures
In the XYZ technique, Gonzalez1 defined the X point as corresponding to the muscle incision performed near the sacrum-coccyx. The Y point corresponds to the most cranial point of the G line. Point Z corresponds to the most caudal point of the G line, tangent to the posterolateral side of the trochanter. The G line corresponds to the lateral limit of the gluteus maximus muscle, with a cephalic portion located 4cm from the superior-posterior iliac spine, over the iliac crest, and with the caudal end defined by the posterolateral side of the trochanter.
With the patient standing, line A is marked, corresponding to the top of the intergluteal crease (Figure 1).

Figure 1. Line A mark.
The entire surgery is based on the following three reference points: the iliac crest, superior-posterior iliac spine, and trochanter. From line A downward, over the intergluteal cleft, a 7cm long and 4mm wide double strip is drawn to mark the sacrocutaneous ligaments, which are responsible for the formation of the intergluteal cleft, for preservation. Next, an inverted heart is drawn, centered in the previously drawn fusiform incision. The lateral ends of the inverted heart are 7cm away from the intergluteal cleft (Figure 2). The entire area corresponding to the inverted heart is infiltrated with a solution containing a vasoconstrictor drug. A skin incision is made, with particular care to preserve the sacrocutaneous ligaments. The subcutaneous plane is then dissected at 45º until reaching the muscle and fascia. The dissection progresses over the muscle and fascia throughout the entire inverted heart. The muscle and fascia are opened, following the direction of the muscle fibers, from the border of the sacrum to the bottom of the detached area, with a 6-cm incision. The index finger is used to create a cleft through the incision. Point X is identified inside the incision by palpating the sacral tuberous ligament, which corresponds to the midpoint of the muscle thickness of approximately 2.5cm deep. A detacher is introduced in point X and follows the direction of the superior-posterior iliac spine. After reaching the anatomical structure, a slight inferior rotation is performed toward point Y. The muscle fibers of the incision are then used as supporting structures in the proximity of the sacrum, and a rotation movement is performed with the tip of the detacher, from point Y until the most caudal end of the G line (point Z), tangent to the posterolateral side of the trochanter (Figure 3). To complete the detachment procedure, both the fingers and a muscle diffuser are used. Drains are placed, implants are inserted, and the muscle incisions are closed with 2-0 nylon sutures. In the inverted heart region, adhesion points are created with Vicryl 3-0 suture. The base of the sacrocutaneous ligaments are closed by using 2-0 nylon suture. The epidermis is stripped and closed from the deep dermis by using 4-0 nylon suture. For epidermal closure, 6-0 nylon suture is used.

Figure 2. Drawing of the inverted heart that guides detachment and exposure of the gluteal fascia.
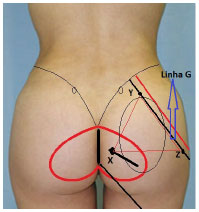
Figure 3. Reference points for intramuscular detachment.
Vergara and Marcos3 did not provide detailed descriptions of the levels and limits of the detachments. The authors described the same type of presurgical marking as that used by Gonzallez-Ulloa to mark the location of the implant, with the patient in the standing and sitting positions. However, when the patient was in the surgical position, the skin changed its relative position, and all of the previous marks were no longer useful to determine the exact implant site. The upper (iliac crest) and lower limits (infragluteal crease) of the area to undergo surgery were marked. The infragluteal crease was marked as the lower limit to assure that the structure was preserved in order to avoid ptosis of the gluteus and delocalization of the implant. The area between the iliac crest and infragluteal crease was divided into three equal parts, with the upper third untouched, the middle third marked for implant placement, and the lower third left to rest in relation to the supporting area (the hamstring) that holds the body weight in sitting position. The lateral location of the implants was marked 4cm away from the intergluteal crease on both sides (Figure 4). An incision of 6 to 7cm was performed in the intergluteal crease, 4cm above the anus or 2cm above the mucocutaneous junction. The incision deepened through the layer of fat located at the presacral fascia. The dissection ran superficially to the fascia, for approximately 3 to 4cm, until reaching the gluteus maximus muscle. Another incision of 6 to 7cm was performed in the aponeurosis of the gluteus maximus muscle, and the intramuscular dissection was performed by using a dissector to create a space between the fascia of the muscle. The incision was performed in the middle of the muscles, 2 to 3cm deep, so that the muscle fibers found above, below, and behind the implant can be used to completely cover it. Drains are placed in the intramuscular pocket.
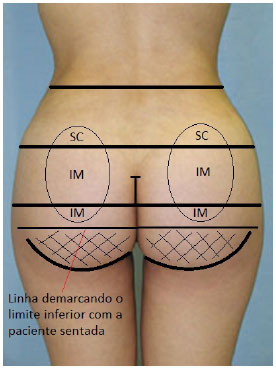
Figure 4. Presurgical markings by Vergara and Marcos (1996).
Mendieta4 marked a horizontal line that linked the tip of the coccyx to the greater trochanter, which then became the lower limit during muscle detachment. The intergluteal incision line was 7 to 8cm long and started from the tip of the coccyx, running upward. To identify the extension of the dissection, the implant was marked above the buttock so that its lower border remains above or just below the horizontal line. The middle region of the implant was located approximately 6 to 7cm away from the sacral middle line. After the incision at the middle line, subcutaneous detachment was performed, thus exposing enough of the muscle fascia to allow the implant to penetrate 7cm into it. The fascia was cut in the direction of the muscle fibers, and an intramuscular dissection of 3cm was performed according to the shape of the implant. After placing the implant, the pocket was closed by using Vicryl 2-0 suture. Drains were placed only in the subcutaneous pocket.
Senderoff5 made a 7cm long incision to the sacral fascia. The subcutaneous detachment was performed laterally up to 7cm of the middle line, exposing the fascia of the gluteus maximus muscle, which was then cut. The incision in the muscle was parallel to the orientation of its fibers and followed by the formation of the implant pocket between the fibers. The implants were placed after hemostasis.
OBJECTIVE
The aim of this study was to discuss the published surgical procedures of augmentation gluteoplasty that uses the intramuscular plane as the implant insertion route. In addition, patients' degree of satisfaction with the results, and the safety, applicability, and reproducibility of the techniques were evaluated.
METHOD
This study consisted of a literature review performed through an electronic bibliographical search on the MEDLINE database in November 2001, using the following keywords: "intramuscular," "gluteal, and "implants." The inclusion criteria were papers that were published in English between 1996 and 2011, and focused on the use of gluteal intramuscular implants in augmentation gluteoplasty.
The search retrieved 11 articles that were examined according to the inclusion criteria. One of the articles was excluded because it did not focus on the relevant subject. The articles were classified as either original research or case reports.
RESULTS
The most frequent immediate complications were pain, wound dehiscence, seroma, and infection (Figure 5). The most commonly reported late complications were muscle atrophy (when the detachment is not well oriented and only one fine layer of muscle remains) and implant rotation due to late formation of the pocket; both complications can lead to perceptible implants.
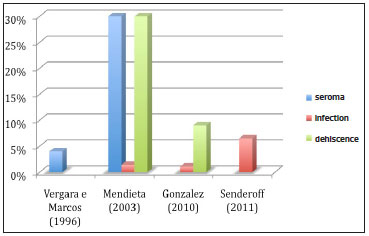
Figure 5. Incidence of complications.
Gonzalez1 reported that all of the patients were satisfied with the results and that the most frequent complaint was pain in the immediate postoperative period, mostly during the first 24h. Three cases of infection were reported among the first 35 cases. In two of the cases, the infection occurred approximately 15 days after the surgery and was preceded by spontaneous drainage of the seroma through the incision. The procedure led to wound dehiscence and later to infection. The preservation of the sacrocutaneous ligaments, the systematic use of drainage and suction for 24 to 48 h, and use of a patch to isolate the anal region during the surgery allowed the surgeons to overcome the reported problems.
Vergara and Marcos3 reported complications in 16 (10%) of 160 patients. Seroma was observed in 7 patients (4%); asymmetry, in 4 (2.66%); capsular contracture, in 3 (2%); hypercorrection, in 1 (0.66%); and implant burst, in 1 (0.66%).
Mendieta4 performed 73 procedures, with high patient satisfaction. The most commonly observed complication, which occurred in 30% of the patients, was wound dehiscence with persisting drainage of the seroma at 8 to 14 days after surgery. One patient had an infection, which did not compromise the implant.
Senderoff5 performed 46 procedures with the use of muscle pockets for a period of 8 years. Seroma was the most frequently reported complication and occurred more frequently in the patients in the subfascial group, when compared with the intramuscular group. Infection occurred in 3 patients in the intramuscular group and in 10 patients in the subfascial group (6.5% for both groups). The causative bacterium most frequently detected was Staphylococcus aureus, present in 11 of the 13 patients. In one of the cultures, Escherichia coli was detected. Pain was the most frequent complaint among the patients in the intramuscular group.
Gonzalez6 did not report late seroma or capsular contracture after the use of smooth or quartz microtextured implants (Silimed, Sientra, Inc, Rio de Janeiro, Brazil). Textured implants, however, were often associated with a high incidence of late seroma. Among the 1046 procedures performed since 1986, the incidence of dehiscence decreased from 14% to less than 10% (in the last 500 procedures performed), and only 1 patient had to undergo a second surgery owing to infection. Of the 11 cases with infection (1.051%), 8 were resolved by cleaning the affected area and removing the debris under general anesthesia, in addition to resterilization of the implant or replacement with a new implant. There were no reported cases of muscle atrophy.
Tavares Filho7 reported promising and reproducible results when using gluteal dermolipectomy with or without dermal fat flaps but with the use of gluteal implants in either the submuscular or intramuscular plane, after a massive weight loss. No complications were reported.
DISCUSSION
The best augmentation gluteoplasty results were obtained when the implants were inserted in the intramuscular plane because these could be covered with a musculocutaneous flap, which is used to maintain the position of the implant and create smooth, symmetrical, esthetically pleasant, and flawless curves. Implants in the subcutaneous or subfascial plane are associated with complications such as seromas, capsular contractures, detachment, and perceptible implant edges.
In the submuscular plane, owing to the proximity of the sciatic nerve, the caudal detachment should not extend beyond the inferior border of the pyramidalis muscle, which limits the location of the implant pocket to the upper gluteal area, with the risk of assuming the shape of a double buttock, especially in patients with long buttocks. In the intramuscular plane, the coverage provided is sufficient to hide the implant.
Gonzalez1 described the XYZ technique, which through the identification of anatomical reference points, guides the surgeon during the identification of the ideal plane for muscle dissection and leads to assertive results, with low complication rates. The intramuscular plane was introduced by Vergara and Marcos3 with the aim of positioning the implant in a lower region; however, anatomical references were not established for a safe intramuscular detachment.
The intramuscular plane has the following disadvantages: difficult muscular detachment in the ideal plane, which can lead to perceptible and palpable implants, and intense pain in the immediate postoperative period. This procedure is not indicated in cases with hypotrophy and intense fibrosis of the gluteus maximus muscle, with the subfascial plane being the first choice in such cases.
The most frequent immediate complications were pain, wound dehiscence, seroma, and infection. Seroma can arise as a consequence of the dissected pocket and the suprafascial detachment performed to expose the muscle in the inverted heart area, and can be due to liposuction of the surrounding regions. Seromas and inverted borders that cause micronecrosis are the main source of wound dehiscence. Preserving the sacrocutaneous ligament when closing the incision in the XYZ procedure prevents damage of the intergluteal crease, improves the cicatrizing process, reduces the risk and severity of wound dehiscence, and provides a platform where the two dehiscent sides can be anchored in case a new suture needs to be performed.
Gonzalez8 recommends dorsal decubitus and the use of special pillows to avoid compression of the detached muscle between the implant and the bed, thus preventing pain at the sciatic nerve, generated by irritation of the nerve, which is caused by serous secretions and bleeding at the site of the pocket detachment.
Gluteal implants can be round or oval, filled with highly cohesive silicone or made of smooth silicone blocks. Round implants should only be used in patients with short buttocks and should not be recommended to tall patients or patients with long buttocks, as the projection of the implant will focus on the upper and middle regions, whereas the lower third will be insufficiently filled with the implant volume.
Quartz oval implants have multiple indications. They can be placed vertically near the sacrum, with the bulkier region located in the upper third of the buttock, which then becomes adequately filled9,10.
The choice of implant volume depends on the pelvis of the patient and the desired results. Implant volumes range from 200 to 500mL. If the implant is round, smaller volumes should be used, that is, between 220 and 240mL for short patients, and between 270 and 300mL for average-sized patients. Quartz implants allow an increase in volume (350 and 400ml) because these implants have smaller lateral projections. Volumes larger than those described can lead to muscle compression and, ultimately, to atrophy, in which case the implant becomes perceptible. The pocket should contain the implant comfortably and allow muscle synthesis without tension.
CONCLUSION
Augmentation gluteoplasty with silicone implants in the intramuscular plane allows for good muscle coverage and protection against infection, in addition to maintaining the implant location and preventing implant migration downward. This procedure consistently ensures natural results, at the level of not only gluteal augmentation but also gluteal reshaping. The resulting buttocks are rounder and firmer, with smooth, symmetrical, and esthetically pleasing contours, without flaws.
The XYZ technique, with the use of markings for anatomical reference, allows a guided intramuscular dissection in the ideal plane. This leads to a thorough technical understanding, making the procedure easily reproducible, and circumvents complications such as palpable and perceptible implants. Moreover, this procedure has been demonstrated to deliver natural and satisfactory results, with low complication rates.
REFERENCES
1. Gonzalez R. Augmentation gluteoplasty: the XYZ method. Aesthetic Plast Surg. 2004;28(6):417-25.
2. Vergara R, Amezcua H. Intramuscular gluteal implants: 15 years experience. Aesthet Surg J. 2003;23(2):86-91.
3. Vergara R, Marcos M. Intramuscular gluteal implants. Aesthetic Plast Surg. 1996;20(3):259-62.
4. Mendieta CG. Gluteoplasty. Aesthet Surg J. 2003;23(6):441-55.
5. Senderoff DM. Buttock augmentation with solid silicone implants. Aesthet Surg J. 2011;31(3):320-7.
6. Gonzalez R. Gluteal implants: the "XYZ" intramuscular method. Aesthet Surg J. 2010;30(2):256-64.
7. Tavares Filho JM, Franco D, Franco T. Postbariatric buttock contouring with dermolipectomy and gluteal implants. Aesthetic Plast Surg. 2011;35(4):589-92.
8. Gonzalez R. A simple way to avoid sciatic pain after intramuscular gluteal implant. Aesthetic Plast Surg. 2007;31(5):602-3.
9. Mendieta CG. Intramuscular gluteal augmentation technique. Clin Plast Surg. 2006;33(3):423-34.
10. Flores-Lima G. Cutaneous fistulas and acute seroma after subfascial gluteal implants. Aesthetic Plast Surg. 2008;32(5):810-2.
Plastic surgeon, associated member of the Brazilian Society of Plastic Surgery (Sociedade Brasileira de Cirurgia Plástica, SBCP)
Institution: Bahia Hospital Medical Center.
Corresponding author:
Daniel Melo De Azevedo
Centro Médico Hospital da Bahia
Avenida Professor Magalhães Neto, 1681, sala 5017. Pituba
Salvador - BA - Brazil - CEP: 41810-011
E-mail: danihelmeloazevedo@hotmail.com
Article received: June 21, 2012
Article accepted: October 15, 2012
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket