



Case Report - Year 2026 - Volume 41Issue 1
Buried Penis Reconstruction after Botched Circumcision: A Multidisciplinary Approach - Case Report
Reconstrução de pênis oculto após circuncisão malsucedida: abordagem multidisciplinar - Relato de caso
Miguel Jimenez-Yarza1, ; Luis Ernesto Jimenez-Yarza2; Miguel Jimenez-Puga3; Manuel Marquina-Sanchez4; Manuel A. Marquina-Cruz5
; Luis Ernesto Jimenez-Yarza2; Miguel Jimenez-Puga3; Manuel Marquina-Sanchez4; Manuel A. Marquina-Cruz5
ABSTRACT
Introduction A buried penis is a condition in which a normal-sized penis is obscured by skin, tissue, or fat, reducing its visible and functional length, and causing issues with appearance, hygiene, voiding, and sexual function. The condition, which can be congenital or acquired, is particularly challenging to manage. In adults, obesity is a major factor, though other causes include trauma, infections, and circumcision-related injuries. Surgical intervention is often necessary.
Case presentation We herein present the case of a 79-year-old male patient who developed penis burying following circumcision surgery. The surgical site was marked in the trapezoid suprapubic area for the performance of an escutcheonectomy. The penile shaft was dissected, and a full-thickness skin graft, taken from the excised suprapubic panniculectomy, was secured. A dressing was applied around the penis. By the eighth day, the graft showed good integration, with no infection, and at the onemonth checkup, the graft and donor site had healed well, with adequate penile-shaft exposure.
Discussion A buried penis can cause sexual dysfunction, painful erections, hygiene issues, and psychological distress. Contributing factors include trauma, congenital lymphedema, radical circumcision, and obesity. Treatment focuses on restoring function, often requiring collaboration between a plastic surgeon and a urologist. Surgical approaches depend on individual factors, with full-thickness skin grafts preferred for better cosmetic outcomes.
Conclusion Despite the low rates of graft loss, there is no consensus on the best treatment approach, emphasizing the need for further research. Addressing both physical and psychological aspects, exploring less-invasive treatments, and improving surgical techniques are crucial for better patient outcomes.
Keywords: buried penis; penile reconstruction; circumcision complication; escutcheonectomy; case report
RESUMO
Introdução O pênis oculto ou embutido é umdistúrbio em que umpênis de tamanho normal está coberto por pele, tecido subcutâneo ou gordura, o que reduz o seu comprimento visível e funcional, e compromete a aparência estética, a higiene, a micção e a função sexual. O distúrbio, que pode ser congênito ou adquirido, representa um desafio particular no manejo clínico. Em adultos, a obesidade é o principal fator associado, embora causas como trauma, infecções e lesões relacionadas à circuncisão também estejam implicadas. A maioria dos casos requer intervenção cirúrgica.
Relato de caso Este artigo apresenta o caso de um paciente do sexo masculino, de 79 anos, que desenvolveu pênis oculto após cirurgia de circuncisão. A área cirúrgica foi demarcada na região trapezoidal suprapúbica para a realização de escuteonectomia. O eixo peniano foi dissecado, e um enxerto de pele total, obtido a partir da paniculectomia suprapúbica ressecada, foi fixado. Um curativo foi aplicado em volta do pênis. No oitavo dia de pós-operatório, observou-se boa integração do enxerto, sem sinais de infecção. À avaliação um mês após a cirurgia, o enxerto e o sítio doador estavam bem cicatrizados, com exposição adequada do eixo peniano.
Discussão O pênis oculto pode causar disfunção sexual, ereções dolorosas, dificuldades de higiene e sofrimento psicológico. Entre os fatores predisponentes estão traumas, linfedema congênito, circuncisão radical e obesidade. O tratamento se centra na restauração funcional e frequentemente exige colaboração entre o cirurgião plástico e o urologista. A escolha da abordagem cirúrgica depende de fatores individuais, sendo os enxertos de pele total preferidos, por oferecerem melhores resultados estéticos.
Conclusão Apesar das baixas taxas de perda de enxerto, ainda não há consenso sobre a melhor técnica terapêutica, o que reforça a necessidade de mais estudos. Abordar os aspectos físicos e psicológicos, explorar opções menos invasivas e aperfeiçoar as técnicas cirúrgicas são medidas essenciais para melhorar os desfechos clínicos.
Palavras-chave: pênis oculto; reconstrução peniana; circuncisão, complicação; escuteonectomia; relato de caso
Introduction
A buried penis refers to a normal-sized phallus that is obscured by skin, subcutaneous tissue, and/or fat in the prepubic area. This condition often leads to reduced visible and functional length of the penis, resulting in patient dissatisfaction related to cosmetic appearance, hygiene, voiding, and sexual function. The condition can also lead to phimosis, which may cause spraying, dribbling, urinary soilage, and skin breakdown. Documenting the degree of patient discomfort and their primary concerns is important. Are they focused on cosmetic outcomes or functional issues? Is their goal to void while standing or to resume sexual activity?1
The syndrome of buried penis in men is generally consid-ered an uncommon condition that is challenging to manage. Various external factors may contribute to this condition in adulthood, which is distinct from conditions like penoscrotal webbing or micropenis. Unlike patients with micropenis, those with a buried penis have a normal corporeal length. The etiology of a buried penis can be congenital or acquired. Congenital cases are often linked to genetic alterations of the Dartos fascia and typically affect pediatric populations. In adults, obesity is a significant contributing factor in most cases.2 The acquired causes include local trauma, recurrent infections, periscrotal lymphedema, and obesity.3 Another potential cause in adult and pediatric patients is circumci-sion-related injury, sometimes referred to as radical circumcision, in which the suture line contracts during heal-ing, forming a cicatrix that traps the penis as it is pushed proximally into the suprapubic fat.2
The incidence of buried penis in adulthood is unknown, and many cases likely go unreported. The literature identifies several specific causes in adults, including abdominoplasty with aggressive release of Dartos fascia attachments to the Scarpa’s fascia, penile lengthening procedures using an ill-advised large pubic V-Y advancement flap, or other genito-inguinal surgeries. Thus, iatrogenic factors are a nontrivial cause of this condition in adults.4
Unfortunately, weight loss alone is often insufficient, and definitive treatment typically requires surgical interven-tion.5 Since 1986, various attempts have been made to classify this condition. Maizels et al.6 proposed a classifica-tion system aimed at simplifying treatment, identifying three subgroups: buried penis, webbed or membranous penis, and trapped penis. A buried penis is a normal-sized phallus hidden within pubic tissue due to inadequate skin fixation at the base of the penis. In a webbed or membranous penis, the penoscrotal angle disappears due to an abnormal distal extension of scrotal skin along the ventral side of the penis. A trapped penis usually results from scarring after penile surgery, such as circumcisions performed on hidden penises.6 The primary treatment goal for all these conditions is to reestablish the fixation of penile skin to the Buck’s fascia, thereby restoring both the penopubic and penoscrotal angles.7 More recently, Pariser et al.8 proposed a classifica-tion system to stratify buried penis repair by complexity, categorizing repairs into the following: I -penile unburying with local skin flap; II -use of a skin graft; III -scrotal surgery; IV -escutcheonectomy; and V -abdominal panniculectomy. Additionally, Mirastschijski9 introduced a classification sys-tem for the adult buried penis based on the location of the glans and penile shaft relative to the surrounding soft tissue. Type-1 patients have excess tissue covering the shaft without invagination; type 2 involves partial invagination; and, in type 3, complete invagination occurs, with manual exposure of the glans or shaft being impossible.9
A thorough examination of abdominal and suprapubic fat is crucial in planning the appropriate surgical approach. The patient should be examined while standing to assess the potential impact of a pannus draping over the genitalia. A genital examination is also necessary to evaluate the prepuce for phimosis and balanitis. In cases of buried penis, the phallus is often palpable beneath the skin.2
The incidence of adult buried penis is on the rise, but there is no consensus regarding a single surgical technique.3 Common operative techniques generally involve the follow-ing steps: a dorsal slit to expose the glans, degloving of the diseased penile skin, escutcheonectomy with or without panniculectomy, and harvesting and application of a split-thickness skin graft (STSG).5 However, full-thickness skin grafts (FTSGs) for penile shaft tissue have shown excellent results, with improved cosmesis, better wound healing, and minimal complications compared to traditional STSGs. Ad-ditionally, using FTSGs can avoid donor-site morbidity.7
While the anterior thigh is a commonly used donor site for STSGs, it carries the risk of donor-site morbidity. An alternative donor site that avoids creating a second defect is the panniculus.10
Case Presentation
We herein present the case of a 79-year-old male patient without any relevant previous medical history who, 7 months prior, had undergone circumcision surgery. Fol-lowing the procedure, he presented with penis burying and scar formation and retraction of the penis shaft. While the patient reported normal urinary function, his chief concern was restoring sexual function. Before starting the procedure, the surgical site was marked in the trapezoid suprapubic area, with the lower part of the incision positioned 2 cm from the base of the penis, in the midline, to enable the skin to be brought closer to the pubic symphysis (►Fig. 1). The patient underwent surgery under general anesthesia followed by an escutcheonectomy. The fascia near the base of the penis was attached to the periosteum of the pubic symphysis using a single nylon 2-0 stitch to enhance penile-shaft exposure.


The penile shaft was then dissected above the Colles fascia (►Fig. 2). An FTSG was taken from the excised suprapubic panniculectomy and was secured with 4-0 catgut sutures, extending from the base of the penis to the healthy skin, with the distal end fixed near the glans (►Fig. 3).
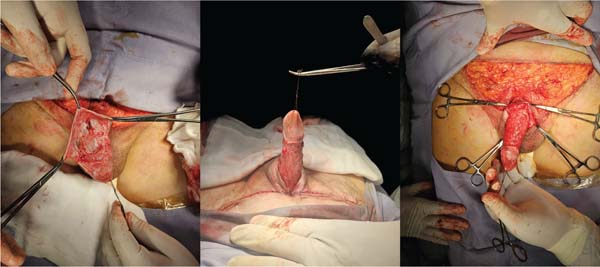





The suprapubic site was closed with simple 2-0 polyglac-tin 910 stitches, and the overlying skin was sutured with 3-0 nylon. A brown-type dressing was applied around the cir-cumference of the penis, with gauze placed over a layer of petroleum jelly mixed with gentamicin (►Fig. 4).
A urinary Foley catheter was left in place until the fifth postoperative day. On the eighth day, the dressing was removed, and the graft showed good integration, with no signs of infection. At the 1-month postoperative checkup, the graft was well-integrated, the donor site had healed, and the penile shaft was adequately exposed (►Fig. 5). At the 6-month postoperative follow-up, the suprapubic incision had matured into a fine, inconspicuous scar. The penile shaft remained fully exposed, with stable contour and projection. There were no signs of graft contracture, recurrence of skin redundancy, nor functional impairment (►Fig. 6).




Discussion
The condition of a buried penis is linked to a range of issues, including loss of sexual function, painful erections, poor hygiene, and psychosocial disorders. In adults, several fac-tors can contribute to the development of this condition, such as local trauma, congenital lymphedema, and radical circumcision that leads to scarring and fibrosis. Obesity is a major contributing factor. The primary goal of the treat-ment is to restore urinary and sexual functions, often requiring the combined expertise of a plastic surgeon and a urologist.1
Adult patients with a buried penis can present with a diverse and complex set of issues, making management strategies challenging. In milder cases, improvements may be achieved through dietary changes, weight loss, and less-invasive surgical procedures such as liposuction. Conversely, more severe cases may involve extensive skin changes lead-ing to conditions such as lichen sclerosus, urethral strictures, scar tissue formation, and lymphedema.5
The surgical options to treat a buried penis are varied and must be tailored to each patient. Factors influencing the surgical approach include history of circumcision, the amount of viable preputial and shaft skin, the underlying cause of the condition, the presence of other comorbidities, and the surgeon’s familiarity with different techniques.2 Surgical interventions may involve approaches to the supra-pubic tissue and lower abdomen, such as lipectomy, pan-niculectomy, or abdominoplasty.1
To minimize the need for additional donor-site harvesting and to improve the functional and cosmetic outcomes, the salvage of skin from the resected escutcheon is preferred. Full-thickness skin grafts are generally more cosmetically appealing than STSGs, though they require excellent vascu-larity for successful graft survival.5 Compared to STSGs, FTSGs experience more immediate contracture due to elastin recoil, but less delayed contracture from myofibroblast ac-tivity. The outcomes of penile skin grafting are generally favorable, with partial and complete graft loss occurring in 8% and 3% of the patients respectively.11
The condition of buried penis presents significant chal-lenges for the affected individuals, encompassing both func-tional and esthetic concerns. The interplay between congenital factors and acquired conditions such as obesity or circumcision-related trauma underscores the complexity of managing this disorder. As illustrated by the case herein reported, surgical intervention remains a cornerstone of effective treatment, with the choice of technique tailored to the patient’s specific needs and underlying factors.
Conclusion
Recent improvements in classification systems and surgical methods, including FTSGs, show promise in restoring func-tion and appearance. However, the lack of a consensus on the best surgical approach indicates the need for further re-search and refinement of treatment methods. Addressing the physical and psychological effects of buried penis can improve patient satisfaction and quality of life. Future re-search should focus on determining the true prevalence of this condition, exploring less-invasive treatment options, and enhancing surgical techniques to reduce complications and improve long-term outcomes. Collaboration between urologists and plastic surgeons, with a focus on patient-centered care, is crucial to achieve optimal results for those affected by this challenging condition.
REFERENCES
1. Ho TS, Gelman J. Evaluation and management of adult acquired buried penis. Transl Androl Urol 2018;7(04):618-627. Doi: 10.21037/tau.2018.05.06
2. Pestana IA, Greenfield JM, Walsh M, Donatucci CF, Erdmann D. Management of “buried” penis in adulthood: an overview. Plast Reconstr Surg 2009;124(04):1186-1195. Doi: 10.1097/prs.0b013e3181b5a37f
3. Bachtold GA, Carvalho LE, Welter CD, Bogo MA, Frainer DA. Surgical correction of buried penis with a skin graft: case report. Rev Bras Cir Plást 2022;37(02):245-249. Doi: 10.5935/2177-1235.2022rbcp0039-en
4. Chopra CW, Ayoub NT, Bromfield C, Witt PD. Surgical manage-ment of acquired (cicatricial) buried penis in an adult patient. Ann Plast Surg 2002;49(05):545-549. Doi: 10.1097/00000637-200211000-00017
5. Monn MF, Socas J, Mellon MJ. The Use of Full Thickness Skin Graft Phalloplasty During Adult Acquired Buried Penis Repair. Urology 2019;129:223-227. Doi: 10.1016/j.urology.2019.04.007
6. Maizels M, Zaontz M, Donovan J, Bushnick PN, Firlit CF. Surgical correction of the buried penis: description of a classification system and a technique to correct the disorder. J Urol 1986;136 (1 Pt 2):268-271. Doi: 10.1016/s0022-5347(17)44837-3
7. Rivas S, Romero R, Parente A, Fanjul M, Angulo JM. Simplificación del tratamiento quirúrgico del pene oculto. Actas Urol Esp 2011; 35(05):310-314. Doi: 10.1016/j.acuro.2010.08.007
8. Pariser JJ, Soto-Aviles OE, Miller B, Husainat M, Santucci RA. A Simplified Adult Acquired Buried Penis Repair Classification System With an Analysis of Perioperative Complications and Urethral Stricture Disease. Urology 2018;120:248-252. Doi: 10.1016/j.urology.2018.05.029
9. Mirastschijski U. Classification and Treatment of the Adult Buried Penis. Ann Plast Surg 2018;80(06):653-659. Doi: 10.1097/sap.0000000000001410
10. Kumar T, Patel A, Chaffin AE. Use of Suprapubic Panniculus for Split-Thickness Skin Graft in Buried Penis Repair. Eplasty 2024; 24:e6
11. Demzik A, Peterson C, Figler BD. Skin grafting for penile skin loss. Plast Aesthet Res 2020;7:52. Doi: 10.20517/2347-9264.2020.93
1. Department of General Surgery, Hospital Regional Monterrey - Instituto de Seguridad
y Servicios Sociales de los Trabajadores del Estado, Monterrey, NL, Mexico
2. Department of Urology, Hospital de Alta Especialidad “Centenario de la Revolución
Mexicana” - Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado,
Emiliano Zapata, MOR, Mexico
3. Department of Plastic and Reconstructive Surgery, Clínica Millenium, Aguascalientes,
AGU, Mexico
4. Department of Urology, Hospital Médica Avanzada Contigo (MAC) Aguascalientes, Aguascalientes,
AGU, Mexico
5. Department of Urology, Hospital Médica Avanzada Contigo (MAC) Aguascalientes Norte,
Aguascalientes, AGU, Mexico
Address for correspondence Miguel Jimenez-Yarza, MD, Departamento de Cirugía General, Hospital Regional Monterrey - Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado, Avenida Adolfo López Mateos 122, Colonia Burócratas Federales, Monterrey, NL, 64380, Mexico (e-mail: migueljy17@gmail.com).
Article received: May 29, 2025.
Article accepted: November 24, 2025.
Editor-in-Chief: Dov Charles Goldenberg.
Conflict of Interests
No conflict of interests to disclose.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket