



Review Article - Year 2026 - Volume 41Issue 1
Esthetic Rib Remodeling in Adults: A Systematic Review of Efficacy and Safety
Remodelamento costal estético em adultos: Revisão sistemática de eficácia e segurança
Leonaldo Torres Diniz1, ; Matheus Santana Belém1; Isabela Maria Cândida Ferreira Dornelas2; Bartolomeu Antonio Nascimento Junior3; Jairo Zacchê de Sá4
; Matheus Santana Belém1; Isabela Maria Cândida Ferreira Dornelas2; Bartolomeu Antonio Nascimento Junior3; Jairo Zacchê de Sá4
ABSTRACT
Introduction Esthetic rib remodeling reduces waist circumference, but available evidence remains scarce. Objective To assess the efficacy, safety, and technical feasibility of esthetic rib remodeling in healthy adults.
Materials and Methods Systematic review of Public Medical Literature (PubMed)/ Medlars online (MEDLINE), Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS), and Cochrane Library on April 28, 2025. Two reviewers independently selected the studies. Eleven clinical studies met the inclusion criteria, covering ribextension or Costari (RibXcar), ultrasound-assisted indentation surgery of the torso (UUAIST), rib osteosynthesis stabilization (RIBOSS), ultrasonic ostemodeling for body contouring (ORUS), waistline esthetic slimming by puncture (WASP) and parallel approach, greenstick fracture, and floating-rib resection.
Results Waist reduction ranged from 6 to 13 cm, being higher for RIBOSS. Reported complications included minor burns (n=2), atelectasis (n=2), pneumothorax (n=2 [intraoperative]þ1 [delayed]), prolonged pleural effusion (n=1), mild dehiscence (n=1), and contour asymmetries (n=3).
Conclusion Although these techniques provide short-term cosmetic benefit, the low methodological quality o the studies and absence of long-term functional outcomes prevent definitive conclusions regarding safety, durability, and ideal indications.
Keywords: plastic surgery; cosmetic surgery; thoracic surgery; rib resection; body contouring
RESUMO
Introdução O remodelamento costal estético objetiva reduzir a circunferência da cintura e remodelar o arco costal, mas a evidência disponível permanece limitada.
Objetivo Avaliar a eficácia, segurança e viabilidade técnica do remodelamento costal estético em adultos saudáveis.
Materiais e Métodos: Revisão sistemática nas bases Public Medical Literature (PubMed)/Medlars online (MEDLINE), Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS) e Cochrane Library até 28 de abril de 2025. Dois revisores conduziram triagem independente. Onze estudos atenderam aos critérios de inclusão, contemplando rib-extension or Costari (RibXcar), ultrasound-assisted indentation surgery of the torso (UUAIST), rib osteosynthesis stabilization (RIBOSS), ultrasonic ostemodeling for body contouring (ORUS), waistline esthetic slimming by puncture (WASP) e abordagem paralela, fratura greenstick e ressecção de costelas flutuantes.
Resultados A redução documentada da cintura variou entre 6 e 13 cm, sendo a maior magnitude associada à RIBOSS. As complicações registradas incluíram queimaduras cutâneas (n = 2), atelectasias (n = 2), pneumotórax (n = 2 intraoperatórios + 1 tardio), derrame pleural prolongado (n = 1), deiscência leve (n = 1) e assimetrias (n = 3).
Conclusão As técnicas demonstram benefício estético de curto prazo; porém, a qualidade metodológica dos estudos é baixa e não há avaliação funcional em longo prazo, limitando conclusões sobre segurança, durabilidade e indicações ideais.
Palavras-chave: cirurgia plástica; cirurgia estética; cirurgia torácica; ressecção de costela; contorno corporal
Introduction
Recently, rib remodeling has gained popularity as an esthetic body contouring technique, particularly among patients seeking slimmer waists, enhanced thoracic definition, and a harmonious overall silhouette. Notable techniques described include ultrasound-assisted indentation surgery of the torso (UUAIST), rib osteosynthesis stabilization (RIBOSS), and selective resection of the floating ribs.1–3
Beyond purely esthetic enhancement, a growing number of patients undergo these interventions for specific purposes, such as bodily feminization or aligning thoracic contour with gender identity. As such, rib reduction or remodeling techniques have been employed to reduce the waist-to-hip ratio (WHR) and accentuate traditional feminine features.4 Despite the increasing clinical adoption of these techniques, literature remains scarce, consisting mainly of case series, with no integrated evaluation of the efficacy, safety, and functional impact in healthy adults undergoing procedures solely for esthetic purposes.2
Recent studies indicate that both patients and surgeons have a positive perception of these procedures, with high esthetic satisfaction and low rates of severe short-term events.1–3 However, methodological heterogeneity and the lack of comparative controls and standardized clinical, functional, and esthetic outcomes limit the interpretation of available results and hinder the establishment of these techniques as evidence-based practices.1 Aspects such as postoperative quality of life and subjective perception of improvement remain scarcely addressed, despite the existence of validated scales (e.g., BODY-Q) recommended for measuring psychosocial outcomes.5 Additionally, objective data on functional impact, such as long-term spirometric parameters, remain scarce.1
To the best of our knowledge, this systematic review is the first to exclusively synthesize evidence regarding rib remodeling performed solely for esthetic purposes in healthy adults, comparing techniques, presenting objective ranges of reduction (when reported), and organizing complications according to documented incidence. Unlike previous reviews that included heterogeneous populations or reconstructive contexts, the present study focuses solely on esthetic procedures, allowing a more precise assessment of efficacy and risks. We aim to fill a critical gap by providing a structured synthesis that supports clinical decision-making, guides surgical practice, and informs the development of future guidelines.
Materials and Methods
The present systematic review of the literature adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)6 and the guidelines set by the International Committee of Medical Journal Editors (ICMJE) for preparing scientific manuscripts.
The guiding question was structured using the population, intervention, comparison, outcome (PICO) framework.7 The population (P) included adults with no thoracic disease; the intervention (I) comprised rib remodeling techniques performed for purely esthetic purposes; the comparison (C), when applicable, involved either no intervention or a comparison between different surgical approaches; and the outcomes (O) encompassed waist circumference reduction, WHR, esthetic satisfaction, surgical complications, and technical feasibility.
We conducted a systematic search of Public Medical Literature (PubMed)/Medlars online (MEDLINE), Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS), and the Cochrane Library, covering all available publications up to April 28, 2025. The search strategy combined free terms and descriptors using Boolean operators, including rib remodeling, esthetic rib resection, floating rib removal, waist reduction surgery, rib contouring, body contouring surgery, greenstick fracture, rib osteotomy, rib reshaping, and thoracic feminization. Supplementary Material 1 shows the complete search strategy, including detailed descriptors and Boolean operators for each database.
Inclusion criteria encompassed studies reporting procedures performed exclusively for esthetic purposes, involving adults (≥ 18 years) of any gender or gender identity, with no history or diagnosis of thoracic disease. Eligible studies included those describing greenstick fractures, monocortical osteotomies, piezotomies, or selective resection of floating ribs, with study designs comprising clinical trials (randomized or non-randomized), prospective or retrospective cohorts, or case series with up to five patients.
We included articles reporting at least one of the following outcomes: waist circumference reduction, WHR change, assessment of body symmetry, patient satisfaction, or complication rates. We only considered articles published in English or Spanish that were available as full texts. Exclusion criteria comprised studies with reconstructive purposes, populations under 18 years, patients with thoracic or significant pulmonary disease, cases of functional thoracic reconstruction, series with fewer than five patients, and articles not accessible in full text.
Two independent reviewers conducted the screening in two stages: first by reading titles and abstracts, and then by evaluating the full text of potentially eligible studies. The assessment of inter-rater agreement utilized Cohen’s kappa coefficient (κ = 0.82), which indicates a near-perfect level of concordance.
Assessment methods were objective (e.g., measurement of abdominal circumference, WHR, standardized imaging) or subjective (self-reported outcomes, surgeon evaluation, spontaneous satisfaction). Additionally, when applicable, standardized tools for psychosocial assessment in esthetic surgery, such as the BODY-Q, were identified and recorded. Studies were grouped according to the surgical technique employed and primary clinical outcomes. A qualitative analysis was performed, with studies categorized as positive (+) if they demonstrated consistent waist reduction, low complication rates, and high esthetic satisfaction; neutral (0) if results were inconclusive, inconsistent, or limited by methodological shortcomings; and negative (—) if outcomes were unsatisfactory.
The design of each study guided the methodological quality assessment. Evaluation of observational studies followed the Newcastle-Ottawa Scale (NOS),8 while case series analysis adhered to the adapted criteria proposed by Murad et al.9
The final synthesis was narrative due to the heterogeneity in study designs, populations, surgical interventions, and assessment tools, with no meta-analysis. Study screening and selection adhered to the PRISMA framework (►Fig. 1). ►Table 1 outlines the quality classification of included studies based on the NOS and Murad recommendations.

| Study | Design | Tool | N | Follow-up | Outcome measurement | Control group | Bias risk | NOS/Murad score* | Final classification |
|---|---|---|---|---|---|---|---|---|---|
| Cipriani et al.10, 2023 | Case series | Murad | 30 | Insufficient (3 months) | Partially objective (circumference + satisfaction) | No | High | Aug 3 | Low quality |
| Cipriani et al.11, 2024 | Case series | Murad | 100 | NR | NR | No | NR | NR | Not classifiable |
| Donders and Saenz,12 2025 | Case series | Murad | 220 | Adequate (6 months) | Circumference + imaging | No | Moderate | Aug 6 | Moderate quality |
| Valdivieso et al.13, 2024 | Prospective multicenter study | NOS (adapted) | 131 | Adequate | Objective (circumference) + subjective | No | Moderate | Sept 7 | Moderate-to-high quality |
| Villa et al.,14 2025 | Retrospective cohort | NOS | 27 | Insufficient (< 6 months) | Objective | No | High | Sept 5 | Low-to-moderate quality |
| Avilez et al.,16 2025 | Case series | Murad | 120 | Adequate | Objective | No | Moderate | Aug 6 | Moderate quality |
| Perez et al.,15 2023 | Abstract | NR | NR | NR | NR | NR | NR | NR | Not classifiable |
| Kudzaev and Kraiushkin,17 2021 | Case series | Murad | 93 | Only 14 with objective follow-up | Objective for subgroup | No | High | Aug 4 | Low quality |
| Hoyos et al.,20 2023 | Case series | Murad | 15 | Insufficient | Subjective + imaging | No | High | Aug 3 | Low quality |
| Verdugo,18 2022 | Retrospective series | NOS | 104 | NR | Subjective | No | High | NR (no numerical score for NOS) | Low quality |
| Chiu et al.,19 2023 | Case series | Murad | 5 | Insufficient | Objective WHR | No | High | Aug 4 | Low quality |
Abbreviations: NR, not reported; WHR, waist-to-hip ratio.

► Tables 2–3 present the extracted data in an organized manner for descriptive analysis and qualitative synthesis, detailing study characteristics and categorizing key clinical outcomes.
| Study | Objective | Method | Study design | Technique | Outcomes | Complications | Conclusion |
|---|---|---|---|---|---|---|---|
| Cipriani et al.10, 2023 | Evaluate USG RibXcar | Case series, n = 30 | Case series | USG RibXcar | Waist reduction; effect maintained for 3 months | 2 mild skin burns; referred pain | Effective and feasible; imaging is essential for security |
| Cipriani et al.11, 2024 | Validate the “clack” sound as an indicator of fracture | Case series, n = 100 | Case series | RibXcar + ‘clack’ validation | “Clack”heard in 90% of patient; monocortical fracture confirmed by ultrasound in 100% | NR | It is recommended not to use the ‘clack’ sound to indicate the end of the surgery, and to conclude the procedure only ultrasound verification |
| Donders and Saenz,12 2025 | Analyze the effectiveness of RibXcar with HDL | Case series, n = 220 | Case series | RibXcar + HDL | Reduction ranging from 6–11 cm in 6 months; high satisfaction | No severe complications; mild pain managed clinically | Consistent and safe technique, stable effect |
| Valdivieso et al.13, 2024 | Describe the UUAIST technique with HDL | Multicentric series, n = 131 | Case series | UUAIST (fracture + HDL) | Average reduction of ~ 8 cm; 97% satisfaction; low asymmetry | Prolonged pain; 3 asymmetries | Promising; requires monitoring and followup |
| r Villa et al.14, 2025 | Evaluate RIBOSS with titanium plates | Retrospective cohort, n = 27 | Retrospective cohort | RIBOSS (osteotomy + plates) | Average reduction ~ 13 cm | 1 mild dehiscence; mild postoperative pain | Anatomical, effective, but without controls |
| Avilez et al.16, 2025 | Present the ORUS technique | Case series, n = 120 | Case series | ORUS (piezotomy) | Waist circumference reduction from 89– 110 cm to 65–69 cm | 2 symptomatic atelectases | Minimally invasive, safe |
| Perez et al.15, 2023 | UUAIST + RIBOSS esthetic results | Retrospective descriptive study (n not confirmed) | Retrospective descriptive study | UUAIST + RIBOSS | NR | No major complications; reports of prolonged pain and asymmetry associated with not wearing the brace | Safe and reproducible techniques, with the potential for greater waist definition and esthetic benefit |
| Kudzaev and Kraiushkin,17 2021 | Evaluate greenstick fracture with braces | Case series, n = 93 | Case series | Greenstick fracture with braces | Average reduction of 8 cm in a single subgroup of 14 patients | No clinical complications reported | Simple, effective, requires brace |
| Hoyos et al.20, 2023 | Evaluate WASP as an adjunct to liposuction | Case series, n ≈ 15 | Case series | WASP | Improved esthetic contour; (approximate) WHR reduction | 1 pneumothorax; 1 prolonged pleural effusion | Effective, minimally invasive alternative |
| Verdugo,18 2022 | Assess 11th–12th rib resection | Retrospective series, n = 104 | Retrospective series | 11th-12th rib resection | Visible improvement, no objective measurements. | 2 intraoperative pneumothoraces | Moderate esthetic outcome, moderate risk |
| Chiu et al.19, 2023 | Quantify impact by WHR | Case series, n = 5 | Case series | Resection of floating ribs | 7.7% WHR reduction (from 0.78–0.72); high satisfaction | No complications; mild, transient pain. | Promising in transgender subjects, limited |
Abbreviations: HDL, high-definition liposuction; n, sample size; NR, not reported; ORUS, ultrasonic ostemodeling for body contouring; RIBOSS, rib osteotomy with osteosynthesis stabilization; USG, ultrasoundguided; UUAIST, ultrasound- and ultrasonic-assisted indentation surgery of the torso; WASP, waistline esthetic slimming by puncture and parallel approach; WHR, waist-to-hip ratio.

| Study | Technique | Classification | Safety | Satisfaction | Technical feasibility | Esthetic outcome | Recovery | Assessment method | Methodological quality | Technical/ results coherence | Time progression | Identified gaps |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cipriani et al.10, 2023 | USG RibXcar | + | Mild burns + pain | High | High, requires ultrasound guidance | Significant reduction documented | Fast | Objective + subjective | Moderate (30 patients, no control group) | Yes | Short-term (3m) | No functional control; losses to follow-up not reported |
| Ciprianiet al.11, 2024 | RibXcar + ‘clack’ validation | + | No complications reported | NR | High | NR | NR | Intraoperative (ultrasound guidance for fracture and angulation) | Low; incomplete data | No (lack of numerical measurements) | NR | Complete absence of numerical outcomes; inability to interpret efficacy |
| Donders and Saenz,12 2025 | RibXcar + HDL | + | No severe complications; mild pain | High | High | 6 to 11 cm reduction | Good | Imaging + circumference | Moderate | Yes | Short-term (6m) | Combined procedure; isolated effect of the technique not measured |
| Valdivieso et al.13, 2024 | UUAIST (fracture + HDL) | + | Prolonged pain; 3 asymmetries | 97% | High | Average reduction of 8 cm | Good | Clinical measurements | High | Yes | Short-term | Requires monitoring; no functional assessment |
| Villa et al.14, 2025 | RIBOSS (osteotomy + plates) | + | 1 mild dehiscence; mild pain | High | High, plate use | Average reduction of 13 cm | Good | Objective (measurements) | Moderate | Yes | Short-term | No control group; high cost |
| Avilez et al.16, 2025 | ORUS (piezotomy) | + | 2 symptomatic atelectases | High | High | Reduction from 89–110 to 65–69 cm | Good | Clinical measurements | High | Yes | Short-term | No systematic functional assessment |
| Perez et al.15, 2023 | UUAIST + RIBOSS | + | No major complications | High (described textually) | High (described as safe and reproducible) | Esthetic improvement | Fast (specially for RIBOSS) | Subjective | Low | Not verifiable | NR | Lack of objective data; no control group; absence no functional assessment |
| Kudzaev and Kraiushkin,17 2021 | Greenstick fracture with brace | + | No clinical complications | High | High, simple | Average reduction of 8 cm (single subgroup of 14 patients) | Good | Objective measurements | Moderate | Yes | Short-term | No control group; depends on adherence to the brace |
| Hoyos et al.20, 2023 | WASP | + | 1 pneumothorax + 1 pleural effusion | High | High | Objective improvement of the side silhouette. | Fast | Subjective + imaging | Moderate | Yes | Short-term | No control; predominantly subjective evaluation |
| Verdugo,18 2022 | 11th-12th rib resection | 0 | 2 pneumothoraces | High (described, not measured) | High, anatomically complex | Visible (not objective) improvement | Moderate | Subjective | Low | Partial | Short-term | No objective measures; pulmonary risk |
| Chiu et al.19, 2023 | Floating rib resection | + | No complications; mild, transient pain | High | High, direct technique | 7.7% WHR reduction (from 0.78–0.7 | Good | Objective WHR | High | Yes | Short-term | n = 5; short followup |
Notes: + indicates a reported positive result; 0 = neutral result. BODY-Q = Body-Related Quality of Life Questionnaire. “Feasibility” refers to clinical applicability and operational cost; “Technical/results coherence” corresponds to the alignment between the technique’s objective, described execution, and the outcomes obtained. “Short-term” refers to ≤ 6 months of follow-up. HDL, High-definition liposuction; NR, not reported; ORUS, ultrasonic ostemodeling for body contouring; RIBOSS, rib osteotomy with osteosynthesis stabilization; USG, ultrasound-guided; UUAIST, ultrasound- and ultrasonic-assisted indentation surgery of the torso.

As it represents a descriptive review with narrative synthesis and no preplanned meta-analysis, it does not meet the International Prospective Register of Systematic Reviews (PROSPERO)’s prioritization criteria; therefore, we did not register our study in this platform.
Results
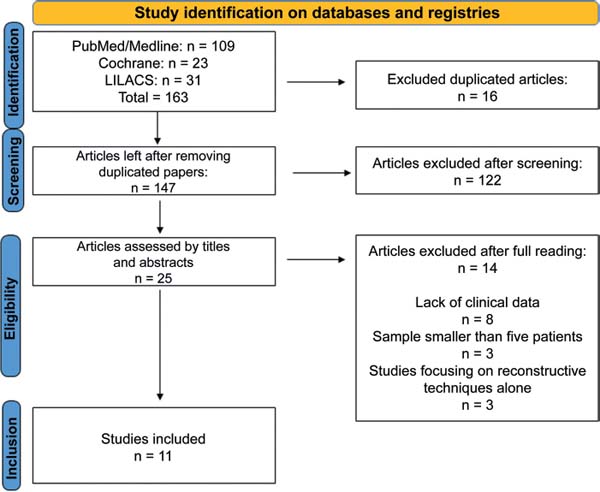
The systematic search identified a total of 163 articles across the 3 electronic databases consulted: PubMed/ MEDLINE (109), LILACS (31), and Cochrane Library (23). After removing 16 duplicates, 147 unique records remained for title and abstract screening. From these papers, we excluded 122 studies as they did not meet the eligibility criteria. We analyzed 25 full-text articles and excluded 14 for various reasons, including the absence of clinical data, a sample size smaller than 5 patients, or the exclusive use of reconstructive techniques. Ultimately, 11 studies met the inclusion criteria and comprised the final sample of this systematic review. ►Table 2 presents a synthesis of the included studies, and ►Fig. 1 shows the PRISMA flowchart.
Three studies evaluated the RibXcar technique (ultrasound-guided monocortical fracture repair), with sample sizes of 30, 100, and 220 patients. In the largest study (n = 220), the documented waist reduction ranged from 6 to 11 cm. These studies reported two minor burns and high esthetic satisfaction. However, satisfaction reports were qualitative, with no objective numerical scale.10 An additional study assessed the intraoperative “clack” marker and demonstrated that only ultrasound confirmed monocortical fractures in 100% of cases, emphasizing the need for realtime imaging.11
Although the largest study (n = 220) reported a measurable reduction, the absence of a control group and potential confounding from concomitant procedures limit the isolated interpretation of the effect.12 A similar approach, the UUAIST technique (n = 131), documented a reduction of up to 8 cm, with satisfaction exceeding 97% and 3 asymmetries recorded as postoperative events.13
Among structural techniques, RIBOSS resulted in reductions of up to 13 cm, the highest ones reported among the available studies. Although one case of minor dehiscence was reported with this technique, no functional follow-up was documented to assess the potential impact.14 In a retrospective series, UUAIST and RIBOSS were frequently performed in combination with high-definition liposculpture (HDL) and other interventions, hindering the ability to isolate the effect of the rib procedures.15
Within the ultrasonic intervention group, the ultrasonic ostemodeling for body contouring (ORUS) technique (n = 120) reported a wide range of reductions between preand postoperative measurements, with two cases of atelectasis documented.16 The greenstick fracture with brace technique (n = 93) documented reductions in a subgroup of 14 patients, with 1 case of non-union, but no reported functional impact.17 ►Table 4 presents a direct comparison of safety across techniques, highlighting the variable event incidence: RibXcar (two burns), ORUS (two atelectases), UUAIST (three asymmetries), RIBOSS (one dehiscence), waistline esthetic slimming by puncture and parallel approach (WASP) (one pneumothorax plus one pleural effusion), and greenstick fracture (one non-union).
| Study | Technique | n (total) | Reported complications | n (cases) |
|---|---|---|---|---|
| Cipriani et al.10, 2023 | USG RibXcar | 30 | 2 mild skin burns + pain | 2 |
| Cipriani et al.11, 2024 | RibXcar (clack) | 100 | NR | NR |
| Donders and Saenz,12 2025 | RibXcar with no incision | 220 | No severe complications; pain not quantified | NR |
| Valdivieso et al.13, 2024 | UUAIST | 131 | Prolonged pain + 3 contour asymmetries (number of pain cases not reported) | 3 |
| Villa et al.14, 2025 | RIBOSS | 27 | 1 dehiscence + 1 mild pain | 2 |
| Avilez et al.16, 2025 | ORUS | 120 | 2 symptomatic atelectases | 2 |
| Perez et al.15, 2023 | UUAIST + RIBOSS | NR | NR | NR |
| Kudzaev and Kraiushkin,17 2021 | Greenstick fracture with brace | 93 | No clinical complications reported | 0 |
| Hoyos et al.20, 2023 | WASP | 15 | 1 pneumothorax + 1 prolonged pleural effusion | 2 |
| Verdugo,18 2022 | 11th–12th rib resection | 104 | 2 intraoperative pneumothoraces | 2 |
| Chiu et al.19, 2023 | Floating rib resection | 5 | No complications; mild, transient pain | 0 |
Notes: n (cases) = number of cases presenting with complications. “No severe complications” refers to the absence of pneumothorax, infection, bleeding, persistent chronic pain, or need for reoperation, according to the criteria of each study. HDL, High-definition liposuction; NR, not reported; ORUS, ultrasonic ostemodeling for body contouring; RIBOSS, rib osteotomy with osteosynthesis stabilization; USG, ultrasound-guided; UUAIST, ultrasoundand ultrasonic-assisted indentation surgery of the torso; WASP, waistline esthetic slimming by puncture and parallel approach.

Among other minimally invasive approaches, the WASP technique (n = 15) reduced lateralization of the costal margin, resulting in high patient satisfaction and no significant complications. Complete rib resection (n = 104) was associated with 2 intraoperative pneumothoraces. However, the lack of reports on objective waist circumference measurements limits the assessment of efficacy.18
Although 1 series (n = 5) documented a 7.7% reduction in WHR, the small sample size limits the interpretability of this finding.19
In summary, reported reductions across techniques ranged from 6 to 13 cm, with the highest reductions having been reported following RIBOSS. However, the absence of control groups, methodological heterogeneity, and lack of standardized functional evaluation limit the ability to draw definitive conclusions.
Qualitative synthesis of included studies
The comparative synthesis highlights that RIBOSS achieved the greatest reductions (up to 13 cm), while minimally invasive techniques showed smaller reductions (6–8 cm). Respiratory events were most frequent with the WASP technique (one pneumothorax and one pleural effusion), whereas UUAIST presented the highest number of asymmetries (three cases). Most studies reported high patient satisfaction; however, few employed validated instruments (e.g., BODY-Q), and no study performed objective long-term functional assessments.
Overall study classification Among the 11 studies evaluated, 9 (81.8%) received a positive classification10–17,20 by demonstrating favorable outcomes in terms of safety, technical feasibility, and patient satisfaction. Two studies (18.2%) were classified as neutral,18,19 and no study received a negative classification, suggesting an initially favorable outlook for esthetic rib remodeling, albeit limited by methodological weaknesses.
Patient safety and satisfaction
All positive studies reported high safety, with no severe complications,10,12,20 only documenting minor events, such as one case of mild dehiscence,14 two cases of mild atelectasis,16 and one seroma.15 A single case of non-union occurred in the brace-assisted technique, without reported functional impact.17 Patient satisfaction was high in 100% of the studies with a positive classification.
Studies with a neutral classification reported two mild pneumothoraces18 in association with complete rib resection. One study reported high satisfaction in terms of WHR reduction.19
Technical feasibility and esthetic appearance
Most studies (n = 9) reported high technical feasibility, describing the methods as safe, reproducible, easy to perform, or minimally invasive.10–16,19,20 A single study described the high anatomical complexity in resecting the 11th and 12th ribs.18
Regarding esthetic appearance, all positive studies reported objective reductions in waist circumference or clinically and esthetically significant measurements. Results from neutral studies were more variable or subjective.
Recovery and assessment methods
For positive studies, recovery time was short and complication-free.10,13,17,20 Two other studies14,16 indicated the need for longer follow-up due to plate implantation or ultrasound use. After complete resection, improvement was visible after 40 days, with no reports of objective measurements.18 Most studies (n = 6) used objective assessments (including circumference and standardized imaging).10–16
Methodological quality and gaps
Methodological quality was high for seven studies,10–13,16,17 moderate for three,14,15,20 and partial for one study.1
The main identified gaps included the lack of a control group,10,15–17,20 short follow-up times (in most studies), and the absence of standardized functional assessments.
► Table 5 summarizes the main anthropometric outcomes of waist circumference and WHR from the 11 studies. When available, we included measures of dispersion (standard deviation and interquartile ranges) and reduction ranges; studies not presenting numerical data were referred to as not reported (NR).
| Study | Technique | n | Anthropometric measurement | Preoperative value | Postoperative value (time) | Reduction | Reported dispersion |
|---|---|---|---|---|---|---|---|
| Cipriani et al.10, 2023 | RibXcar (USG monocortical fracture with no incision) | 30 | Waist circumference (cm) | NR | NR | Waist reduction described only qualitatively, with no average values or numerical ranges | NR |
| Cipriani et al.11, 2024 | RibXcar with ‘clack’ validation (tactile feedback) | ~ 100 | Waist circumference (cm) | NR | NR | Waist reduction and ‘clack’ maintenance, but with no complete numerical values | NR |
| Donders and Saenz,12 2025 | RibXcar + HDL (no incision) | 220 | Waist circumference (cm) | Preoperative average = 77.92 cm | Postoperative average = 66.18 cm (6 months) | The authors reported a reduction ranging from 6–11 cm in waist circumference at 6 months of follow-up | Reduction range of 6 to 11 cm; no SD, IQR or CI are provided for waist measurement |
| Valdivieso et al.13, 2024 | UUAIST (corticotomy with piezotome + HDL) | 131 | Waist circumference (cm) | Preoperative median = 72 cm (IQR, 6 cm) | Postoperative median= 65 cm (IQR, 5 cm) at 3 months | Median reduction = 8 cm (IQR, 4.5 cm); subgroup with rib remodeling only: median = 7 cm (IQR, 3 cm); subgroup with remodeling + liposuction/associated procedures: median = 9 cm (IQR, 4 cm) | IQR reported for preand posttreatment values and for the difference (4.5 cm overall; 3 cm in group 1; 4 cm in group 2) |
| Villa et al.14, 2025 | RIBOSS (greenstick osteotomy + titanium plate) | 27 | Waist circumference (cm) | Preoperative average = 80.8 cm | 68.8 cm in 1 month; 67.8 cm in 3 months | Average reduction = 12.1 cm in 1 month and 13.0 cm in 3 months; minimum reduction = 8 cm; reduction = maximum 18 cm. | Only average values and range (8 to 18 cm) are provided; the article does not report specific SD, IQR, or CI for waist circumference |
| Avilez et al.16, 2025 | ORUS | 120 | Waist circumference (cm) | Pre-operative median value = 81-83 cm (10-90 percentiles: 70 to 96 cm)* | 90-day median value = 65-67 cm | Documented reduction = 7–26 cm, with median values of 13 cm for ORUS and 15 cm for (ORUS + liposuction | 10–90 percentiles for preoperative values; SD and IQR values not reported |
| Perez et al.15, 2023 | UUAIST + RIBOSS (preliminary series, conference summary) | Not confirmed | Waist circumference/WHR | NR | NR | Waist reduction of up to approximately 12 cm in some cases | NR |
| Kudzaev and Kraiushkin,17 2021 | Greenstick fracture of 11th–12th ribs + brace | 93 (14 at ≥ 6 months follow-up) | Waist circumference (cm) | Aggregated values are not reported; the article focuses on differences | Absolute values not reported, only ranges | In 14 patients with ≥ 6-month follow-up: average reduction = ~8.0 cm in waist circumference, ranging from 4 to 15 cm | Mean and range (4– 15 cm); DP, IQR, and CI for this variable are not reported |
| Hoyos et al.20, 2023 | WASP (minimally invasive bone remodeling as a complement to liposuction) | ~ 15 | Primarily WHR and visual esthetic assessment. | NR | NR | The authors report a descriptive esthetic improvement in contour and a WHR reduction; however, there is no table with average values or detailed numerical dispersion | NR |
| Verdugo,18 2022 | 11th–12th rib resection + liposuction/abdominoplasty | 104 | Waist circumference (cm) | NR | NR | Retrospective series; the text describes “visible” improvement in waist circumference, but no average circumference or WHR values as tables | NR |
| Chiu et al.19, 2023 | 11th–12th floating rib resection | 5 | WHR | Preoperative mean WHR = 0.78 ± 0.04 | Postoperative mean WHR = 0.72 ± 0.06 in 3 months | WHR average reduction = 7.7% WHR (individual variation from 4.8–10.9%) | SD reported for WHR (±0 .04 and ± 0.06) and percentage change (7.7 ± 2.4%); no aggregatecircumference in cm |
Abbreviations: HDL, high-definition liposuction; CI, confidence interval; IQR, interquartile range; NR, not reported; ORUS, ultrasonic ostemodeling for body contouring; RIBOSS, rib osteotomy with osteosynthesis stabilization; SD, standard deviation; USG, ultrasound-guided; UUAIST, ultrasound- and ultrasonic-assisted indentation surgery of the torso; WASP, waistline esthetic slimming by puncture and parallel approach; WHR, waist-to-hip ratio. Percentile values refer to the ranges described in the original articles.

Discussion
The current review shows that, although esthetic rib remodeling has gained popularity as a body-contouring alternative, the available scientific evidence remains scarce and methodologically weak. Most studies had observational designs, primarily as case series, which lacked control groups and included small sample sizes. These limitations hinder definitive conclusions about the long-term (i.e., over 12 months) efficacy and safety.1,2 Interpretation of findings is further complicated by the heterogeneity of techniques—RibXcar, UUAIST, RIBOSS, ORUS, WASP, greenstick fracture, and floating rib resection—with variable short-term results and non-standardized outcomes.1,2,21
Observed effectiveness is mainly concentrated in the short term (fewer than 6 months). Documented reductions in abdominal circumference ranged from 6 to 13 cm, with the greatest decrease associated with the RIBOSS technique.21 When assessed, WHR showed a mean reduction of 7.7%; however, this outcome was measured in only one study.1 A major limitation is the lack of objective functional assessments, such as spirometry, chronic pain evaluation, and thoracic mobility, which represents a critical gap. This is particularly relevant given that other procedures involving rib manipulation have measurable respiratory effects, and remodeling techniques may involve osteotomy and resection.22–25
Although safety seems acceptable in the short term, this assumption relies on fragmented and heterogeneous data. Reported adverse events included the following: two burns with RibXcar; three asymmetries with UUAIST; one wound dehiscence with RIBOSS; two cases of atelectasis with ORUS; one pneumothorax and one pleural effusion with WASP; no complications in the greenstick fracture series; and 2 intraoperative pneumothoraces in the 11th to 12th rib resection technique.1,2,21 In several publications, information on complications was insufficient or absent, preventing accurate estimation of incidence rates and meaningful risk-benefit comparisons. ►Table 6 summarizes the adverse events reported for each technique as extracted from the included studies.
| Technique | Reported complications |
|---|---|
| RibXcar (USG) | 2 burns |
| RibXcar (clack) | Not informed |
| RibXcar with no incision | No severe complications reported |
| UUAIST | 3 asymmetries, prolonged pain |
| RIBOSS | 1 dehiscence, mild pain |
| ORUS | 2 atelectases |
| Greenstick fracture with brace | No complications; 1 nonunion with no clinical impact |
| WASP | 1 pneumothorax, 1 pleural effusion |
| 11th–12th rib resection | 2 intraoperative pneumothoraces |
| Floating rib resection | No complications |
Abbreviations: ORUS, ultrasonic ostemodeling for body contouring; RIBOSS, rib osteotomy with osteosynthesis stabilization; USG, ultrasound-guided; UUAIST, ultrasoundand ultrasonic-assisted indentation surgery of the torso; WASP, waistline esthetic slimming by puncture and parallel approach.

The absence of psychosocial assessment represents another important limitation. Although validated instruments, such as BODY-Q (measuring satisfaction, self-image, and quality-of-life impact), are available, none of the included studies applied structured psychometric scales to evaluate the actual psychological benefit in healthy patients undergoing esthetic rib remodeling.26 Therefore, it is not possible to determine whether perceived esthetic outcomes correspond to emotional improvement or merely reflect responses to social expectations.
From a bioethical perspective, rib remodeling is an irreversible procedure occasionally performed in healthy subjects. The literature on ethics in esthetic surgery highlights potential vulnerabilities in patient autonomy, influenced by sociocultural factors, particularly in procedures aimed at modifying the body to conform to esthetic ideals.27–29 Additionally, the absence of formal Brazilian or international guidelines on indications, techniques, or follow-up creates ambiguity, placing the responsibility of clinical judgment and patient protection solely on the surgeon.27–29
From a Brazilian perspective, plastic surgery plays a prominent international role, including as a destination for medical tourism.30 However, the lack of procedural regulation by the Brazilian Medicine Board (Conselho Federal de Medicina, CFM, in Portuguese) and Brazilian Society of Plastic Surgery (Sociedade Brasileira de Cirurgia Plástica, SBCP, in Portuguese) allows its performance outside accredited settings, which may increase the risk of complications and compromise the institutional reputation of the specialty.31 The literature further suggests that Brazil has a strategic opportunity to lead the development of the first global ethical and technical guidelines for esthetic rib remodeling, standardizing indications, professional qualifications, and perioperative safety.30,31
In summary, rib remodeling shows immediate esthetic benefits; however, these advantages are backed by weak scientific evidence due to a lack of functional follow-up, psychosocial assessment, limited technical standardization, and a significant regulatory gap. Progress in this field depends on the development of prospective studies, objective functional assessment, the use of psychometric instruments, the establishment of multicenter registries, and the formulation of ethical and regulatory frameworks—ideally led by Brazilian plastic surgery.
Conclusion
The available esthetic rib remodeling techniques demonstrate satisfactory short-term outcomes, with objective reductions in circumference and high patient satisfaction. Nevertheless, the absence of controlled studies, standardized functional assessment, and long-term follow-up precludes definitive conclusions regarding safety, durability, and optimal indications of these procedures.
REFERENCES
1. Danilla S, González-Arestizábal T. Costal surgery for waist improvement safety and efficacy: a systematic review of the literature. Aesthetic Plast Sur Surg 2025;49(02):ePub ahead of print. Available from: Doi: 10.1007/s00266-025-04815-x PubMed
2. Ferreira LM, Bonin GS, Bernardes ABS, et al. Is there scientific evidence on the practice of rib resection or remodeling for body contouring purposes?—a systematic review Aesthetic Plast Surg 2025;49(07):2007–2014. Doi: 10.1007/s00266-025-04685-3
3. Ioppolo L, Borelli F, Bonetti MA, et al. Rib reduction technique in patients with isolated chondrocostal chest wall prominence undergoing breast augmentation. Aesthetic Plast Surg 2024;48 (22):4656–4659. Doi: 10.1007/s00266-024-04006-0
4. Patel H, Samaha Y, Ives G, Lee TY, Cui X, Ray E. Chest Feminization in Male-to-Female Transgender Patients: A Review of Options. Transgend Health 2021;6(05):244–255. Doi: 10.1089/trgh.2020.0057
5. Poulsen L, McEvenue G, Klassen A, Hoogbergen M, Sorensen JA, Pusic A. Patient-Reported Outcome Measures: BODY-Q. Clin Plast Surg 2019;46(01):15–24. Doi: 10.1016/j.cps.2018.08.003
6. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372(71):n71. Doi: 10.1136/bmj.n71
7. Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak 2007;7(01):16. Doi: 10.1186/1472-6947-7-16
8. Wells GA, Shea B, O’Connell D, et al. Newcastle–Ottawa scale (NOS) for assessing the quality of nonrandomised studies in metaanalyses. Ottawa: Ottawa Hospital Research Institute; 2011
9. Murad MH, Sultan S, Haffar S, Bazerbachi F. Methodological quality and synthesis of case series and case reports. BMJ Evid Based Med 2018;23(02):60–63. Doi: 10.1136/bmjebm-2017110853
10. Cipriani RMM, Vega HD, Uribe LC, Viaro M, Adrianzen GA, Botelho DL. Waist Remodeling without Incision, with Ultrasound-guided Monocortical Fracture. Plast Reconstr Surg Glob Open 2023;11 (12):e5499. Doi: 10.1097/GOX.0000000000005499
11. Cipriani RMM. Is “Clack” Enough? Rib Remodeling Guided by Ultrasound. Plast Reconstr Surg Glob Open 2024;12(05):e5843. Doi: 10.1097/GOX.0000000000005843
12. Donders RR, Saenz JR. Waist Remodeling Without Incision, With Ultrasound-guided Monocortical Fracture: Report of 220 Patients. Plast Reconstr Surg Glob Open 2025;13(03):e6595. Doi: 10.1097/GOX.0000000000006595
13. Valdivieso CO, Valdivieso DO, Hoyos AE, et al. Ultrasonic- and Ultrasound-assisted Improvement of Silhouette of the Torso: Bone Structure High-definition Remodeling (Part I). Plast Reconstr Surg Glob Open 2024;12(01):e5513. Doi: 10.1097/GOX.0000000000005513
14. Villa HA, Villabona-Florez SJ, Hoyos AE, Pachon MEP, Serrano-Reyes HM, Sandoval CJD. Aesthetic Rib Cage Remodeling with Osteosynthesis: Body Structural High-Definition Reshaping (Rib Osteotomy with Osteosynthesis Stabilization). Plast Reconstr Surg 2025;155(02):279–288. Doi: 10.1097/PRS.00000000 00011512
15. Perez M, Ariza AH, Aguilar H. High-Definition Rib (HDR) Body Contouring Surgery: UUAIST and RIBOSS. Plast Reconstr Surg Glob Open 2023;11(10):15–16. Doi: 10.1097/01.GOX.0000991928.14101.a9 PubMed
16. Avilez JE, Noriega DR, Martínez CE, Quisilema JM. ORUS: Ultra-sonic Ostemodeling for Body Contouring. Plast Reconstr Surg Glob Open 2025;13(01):e6464. Doi: 10.1097/GOX.0000000000006464
17. Kudzaev KU, Kraiushkin IA. Waist Narrowing without Removal of Ribs. Plast Reconstr Surg Glob Open 2021;9(07):e3680. Doi: 10.1097/GOX.0000000000003680
18. Verdugo JP. Rib removal in body contouring surgery and its influence on the waist. Sci Art Plast Surg J 2022;3(01):8. Doi: 10.47511/sapsj.v3.8144
19. Chiu YH, Chiu YJ, Lee CC, Wang TH, Lee JL. Ant Waist Surgery: Aesthetic Removal of Floating Ribs to Decrease the Waist-hip Ratio. Plast Reconstr Surg Glob Open 2023;11(03):e4852. Doi: 10.1097/GOX.0000000000004852
20. Hoyos AE, Pachon MEP, Duarte P, et al. Waistline Aesthetic Slimming by Puncture and Parallel Approach for Rib Remodeling procedures. Aesthet Surg J Open Forum 2025;7(01):ojaf044. Doi: 10.1093/asjof/ojaf044
21. Milani-Reis A, Mora MMR, Bregion PB, et al. Rib remodeling without rib resection: a systematic review and meta-analysis. Aesthetic Plast Surg 2025;•••: Epub ahead of print. Doi: 10.1007/s00266-025-05240-w
22. Kumar V, Vatkar AJ, Baburaj V, Najjar E, Bansal P. Pulmonary function after thoracoplasty for adolescent idiopathic scoliosis: a systematic review and meta-analysis. Eur Spine J 2022;31(11): 2972–2986. Doi: 10.1007/s00586-022-07375-9 PubMed
23. Bae SY, Park JH, Na B, et al. Thoracic cavity remodeling and pulmonary function change after chest wall resection. J Thorac Dis 2024;16(05):2723–2735. Doi: 10.21037/jtd-24-25
24. Demura S, Kato S, Yoshioka K, et al. The influence of costal resection on pulmonary function after total en bloc spondylectomy for spine tumor. J Orthop Sci 2023;28(05):972–975. Doi: 10.1016/j.bjps.2010.03.034
25. Heuker D, Lengele B, Delecluse V, et al. Subjective and objective assessment of quality of life after chest wall resection. Eur J Cardiothorac Surg 2011;39(01):102–108. Doi: 10.1016/j.ejcts.2010.03.071
26. Klassen AF, Cano SJ, Alderman A, et al. The BODY-Q: A Patient-Reported Outcome Instrument for Weight Loss and Body Contouring Treatments. Plast Reconstr Surg Glob Open 2016;4(04): e679. Doi: 10.1097/GOX.0000000000000665
27. De Roubaix JAM. Beneficence, non-maleficence, distributive justice and respect for patient autonomy–reconcilable ends in aesthetic surgery? J Plast Reconstr Aesthet Surg 2011;64(01): 11–16. Doi: 10.1016/j.bjps.2010.03.034
28. Atiyeh BS, Rubeiz MT, Hayek SN. Aesthetic/Cosmetic Surgery and Ethical Challenges. Aesthetic Plast Surg 2020;44(04):1364–1374. Doi: 10.1007/s00266-020-01821-z
29. Özer M, Mortimore I, Jansma EP, Mullender MG. Labiaplasty: motivation, techniques, and ethics. Nat Rev Urol 2018;15(03): 175–189. Doi: 10.1038/nrurol.2018.1
30. Edmonds A. “Almost invisible scars”: medical tourism to Brazil. Signs (Chic Ill) 2011;36(02):297–302. Doi: 10.1086/655909
31. Oliveira GVd, Cordeiro AAR, Portela LC, et al. Impact of unlawful aesthetic practices in Brazil: a multicenter survey on complications and the need for regulatory reform. Dermatol Surg 2025;48 (09): Epub ahead of print. Doi: 10.1097/DSS.0000000000004774
1. Plastic Surgery Department, Hospital das Clínicas, Universidade Federal de Pernambuco
(HC-UFPE), Recife, PE, Brazil
2. Plastic Surgery Department, Hospital Geral de Vila Penteado Dr. José Pangella,
São Paulo, SP, Brazil
3. University of Toronto, Toronto, ON, Canada
4. Universidade Federal de Pernambuco (UFPE), Recife, PE, Brazil
Address for correspondence LeonaldoTorres Diniz, Avenida Professor Moraes Rego 1.235, Cidade Universitária, Várzea, Recife, PE, 50670– 420, Brazil (e-mail: leonaldotd@gmail.com).
Article received: August 16, 2025.
Article accepted: January 13, 2026.
Conflict of Interests
The authors have no conflict of interests to declare.
Editor-in-Chief: Dov Charles Goldenberg.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket