



Original Article - Year 2026 - Volume 41Issue 1
Surgical Outcome of Fronto-Orbital Advancement Using Less Rigid Fixation on the Anterior Cranial Fossa in Patients with Craniosynostosis
Desfecho cirúrgico do avanço fronto-orbital com fixação menos rígida na fossa craniana anterior em pacientes com craniossinostose
Rebecca Xin Yi Choy1, ; Wan Azman Wan Sulaiman1; Che Zubaidah Bt Che Daud3; Hamidah Mohd Zainal2; Johari Yap Abdullah4
; Wan Azman Wan Sulaiman1; Che Zubaidah Bt Che Daud3; Hamidah Mohd Zainal2; Johari Yap Abdullah4
ABSTRACT
Introduction Craniosynostosis, characterized by the premature fusion of cranial sutures, can lead to increased intracranial pressure, craniofacial abnormalities, and neurodevelopmental concerns. Fronto-orbital advancement (FOA) is a surgical intervention aimed at increasing anterior cranial volume (ACV) and improving frontal cranial symmetry.
Objective To evaluate the outcome on the anterior cranial fossa of patients who underwent less rigid fixation using nonabsorbable nylon 2/0 sutures.
Methods Nonabsorbable nylon 2/0 sutures as fixation method were used in 19 patients with craniosynostosis involving either the coronal or metopic sutures. Their pre- and postoperative volumetric analyses were conducted using three-dimensional (3D) computed tomography (CT) imaging to evaluate the ACV, anterior cranial vault asymmetry index (ACVAI), and change in the head shape using cephalic index (CI) as primary outcome measures.
Results The results demonstrated a significant increase in mean ACV, from 259.15 (SD: 162.61) to 314.38 (SD: 79.78) cm3 postoperatively (p=0.042). Also, there was a notable improvement in symmetry (p=0.05), indicated by a mean ACVAI change from 1.14 (SD: 4.78) to -1.63 (SD: 4.98). However, CI analysis revealed no significant postoperative changes in head shape classification.
Conclusion These findings suggest that FOA with nonabsorbable nylon suture is an effective and cost-efficient method in increasing ACV and improving symmetry while maintaining structural stability, making it a viable option for patients with limited financial resources. However, the lack of significant changes in head shape classification highlights the need for further refinement in surgical techniques. Long-term follow-up and larger cohorts are recommended to assess the persistence of these outcomes and optimize treatment strategies.
Keywords: anterior cranial fossa; craniosynostosis/ surgery; fronto-orbital advancement; nonabsorbable sutures
RESUMO
Introdução A craniossinostose, caracterizada pela fusão prematura das suturas cranianas, pode causar aumento da pressão intracraniana, anomalias craniofaciais e problemas de desenvolvimento neurológico. O avanço fronto-orbital (AFO) é uma intervenção cirúrgica que visa aumentar o volume craniano anterior (VCA) e melhorar a simetria craniana frontal.
Objetivo Avaliar o resultado do AFO na fossa craniana anterior de pacientes submetidos a uma fixação menos rígida com suturas não absorvíveis de nylon 2/0.
Métodos O método de fixação com suturas não absorvíveis de nylon 2/0 foi utilizado em 19 pacientes com craniossinostose e acometimento das suturas coronais ou metópicas. As análises volumétricas pré- e pós-operatórias foram realizadas por meio de tomografia computadorizada (TC) tridimensional (3D) para avaliação do VCA, do índice de assimetria da abóbada craniana anterior (IAACA) e da alteração no formato da cabeça por meio do índice cefálico (IC) como desfechos primários.
Resultados Os resultados demonstraram um aumento significativo no VCA médio de 259,15 (desvio-padrão [DP]: 162,61) para 314,38 (DP: 79,78) cm3 no pós-operatório (p=0,042). Houve uma melhora na simetria (p=0,05), indicada pela alteração do IAACA médio de 1,14 (DP: 4,78) para -1,63 (DP: 4,98). No entanto, a análise de IC não revelou modificações pós-operatórias significativas na classificação do formato da cabeça.
Conclusão Esses achados sugerem que o AFO com sutura não absorvível de nylon é um método eficaz e econômico para aumento do VCA e melhora da simetria, com manutenção da estabilidade estrutural. Assim, o AFOé uma opção viável para pacientes com recursos financeiros limitados. No entanto, a ausência de alterações significativas na classificação do formato da cabeça destaca a necessidade de maior refinamento das técnicas cirúrgicas. Recomenda-se acompanhamento em longo prazo e coortes maiores para avaliação da persistência desses desfechos e otimização das estratégias de tratamento.
Palavras-chave: avanço fronto-orbital; craniossinostose/ cirurgia; fossa craniana anterior; suturas não absorvíveis
Introduction
Craniosynostosis is a condition that is characterized by the premature fusion of one or more cranial sutures. Nonsyndromic craniosynostoses are more common than syndromic ones, with a prevalence of 0.4 to 1 per 1,000 births.1 It can be classified according to the sutures involved or the etiological factor of the condition, which are nonsyndromic with no genetic anomaly, nonsyndromic with a known genetic anomaly, or syndromic. Anatomic classifications can depend on whether a single major suture, single minor one, or multiple sutures are involved, thus being named according to the sutures involved.2
There are many effects of craniosynostosis on a growing child, primarily the increased intracranial pressure. Furthermore, it can also involve the airway, leading to ocular issues, as well as psychosocial and neurodevelopmental delays. Another effect of craniosynostosis is the abnormal head shape of the child, which is commonly an aesthetic concern for parents.
Fusion of the metopic and coronal sutures affect the appearance of the frontal region causing various abnormalities such as asymmetry, triangular forehead, supraorbital retrusion, temporal hollowing and a high prevalence of ocular abnormalities, such as hypertelorism, proptosis, strabismus, and amblyopia.1,3,4 Elevated intracranial pressure may predispose to optic nerve atrophy, located in the anterior cranial fossa.1,5
Fronto-orbital advancement (FOA) is the surgical intervention for craniosynostosis when there is premature closure involving either the metopic or coronal sutures.6–12 It can be done in isolation or with cranial vault remodeling and assist in the anterior expansion of the cranial vault, enabling correction of the deformities and asymmetries to the frontal region.
The surgical correction for craniosynostosis requires multiple osteotomies made in the skull with repositioning of the bone flaps. Historically, these flaps were fixed with metal plates and screws which gradually shifted to absorbable plates and screws to adapt to the growing skull and brain of the child. Fixation with absorbable sutures with the 2-0 polydioxanone first gained its entrance as a method of fixation of bone flaps in craniosynostosis in the year 2000, leading to the use of this “low budget” fixation in surgery with outcomes comparable to those using resorbable plates and screws.13–15
The primary objectives of this study are to evaluate the effects of FOA using nonabsorbable nylon sutures on anterior cranial volume (ACV), symmetry, and head shape in patients with craniosynostosis. By assessing the outcome on the anterior cranial fossa using this technique, we hope to provide valuable insights for clinicians in resource-limited settings and contribute to the ongoing optimization of craniosynostosis management.
Methods
In this retrospective study, nonabsorbable 2/0 nylon sutures were used for bone flap fixation during FOA, in 19 patients with craniosynostosis involving coronal or metopic sutures. The mean age was 29 months at the time of surgery. The procedures took place between the years 2019 and 2023 by two experienced craniofacial surgeons.
The study cohort consisted of a nearly equal gender distribution, comprising 9 males and 10 females. Most participants were of Malay ethnicity (n = 15), followed by Indian (n = 2) and Chinese (n = 1). Multi-suture craniosynostosis was the predominant presentation, observed in 17 patients (89.4%), while single-suture involvement was identified in only 2 cases (10.6%). Additionally, 13 patients (68.4%) were diagnosed with syndromic craniosynostosis, and 6 (31.6%) presented with nonsyndromic forms of the condition.
Operative Technique
The skull was approached with a bicoronal incision, and scalp flap was bilaterally raised in the subperiosteal plane anteriorly to the level of the bilateral supraorbital rims. Dissection was performed to expose and release soft tissues around the superior orbital rim, the lateral orbital rim to level frontozygomatic suture, and medially to the nasal process of the frontal bone. The ventral anterior cranial fossa was then exposed to facilitate fronto-orbital osteotomies.
Posteriorly, the scalp flap was raised according as needed to expose the bitemporoparietal region for cases that required cranial vault remodeling. A supraorbital bandeau was formed by an osteotomized horizontal strip of bone that was reshaped and repositioned forward by a minimum of 15 mm.
A bone graft was used as an inlay strut to anchor the bandeau laterally. (►Fig. 1) An equal number of holes were drilled on opposing bone flaps once positioned, and the less rigid fixation was done with nonabsorbable nylon 2/0 sutures in a crisscross, figure-of-8 fashion to provide stability (►Fig. 2), like cross lacing a corset.16




Depending on the skull dysmorphology, cranial vault remodeling was done with the same method of fixation. A postoperative computed tomography (CT) scan is typically repeated after 3 months and again after 3 years, though the timing may vary depending on patients’ clinical condition.
Analysis of Operative Results
Pre-and postoperative three-dimensional (3D) CT head scans were retrieved from the radiology department’s database in the Digital Imaging Communications in Medicine (DICOM) format and stored digitally. The ACV was measured using the Medical Imaging Interaction Toolkit (MITK, German Cancer Research Center) software, v2023.12, while the anterior cranial vault asymmetry index (ACVAI) and cephalic index (CI) were analyzed using the Mimics Medical (Materialise Inc.) software, v.17.0. All measurements were performed on a Dell Inspiron 14 (Dell Inc.) workstation equipped with an Intel Core i5-7200U CPU (Intel Corp.), with 2.50 GHz and 12.0 GB RAM. The compiled data were organized in an Excel (Microsoft Corp.) sheet for further analysis.
Anterior Cranial Vault (ACV) Volumetric Study
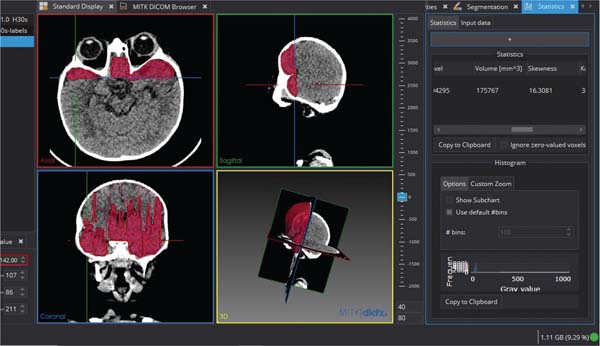
The anterior cranial vault was segmented by selecting the region of interest (ROI) on the sagittal plane. Following that, the region growing method was initiated at a chosen pixel, a seed point, and then manually traced using a computer mouse-driven pointer in each slice of the CT brain image from the sagittal view to achieve the ROI’s border. The segmented area was then interpolated into 3D. The volume of the interpolated area was automatically calculated using the software and displayed in mm3 (►Fig. 3).

Anterior Cranial Vault Asymmetry Index (ACVAI) Calculation
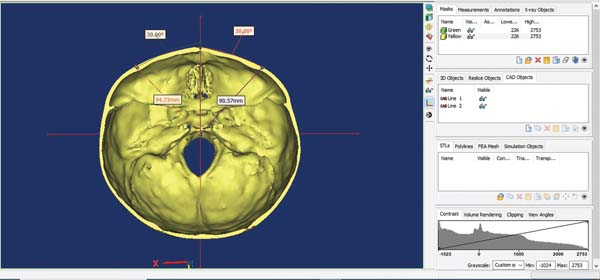
The calculation began with the segmentation of the region of interest, followed by the generation of a 3D image of the skull. The upper portion of the skull was then erased, leaving only the base for analysis. A line connecting the midpoint of the anterior edge of the foramen magnum and the center of the sella turcica was selected as the X-axis, while a vertical line passing through the midpoint (O) of the X-axis was delineated as the Y-axis. The lengths of the two bisectors, AO and BO, were measured, and the ACVAI was calculated using the formula: ACVAI = |AO − BO|/ BO × 100% (►Fig. 4).

Cephalic Index (CI) Calculation
The CI was calculated using axial CT brain images to assess cranial shape. First, the axial slice that showed the widest biparietal diameter (BPD) and the slice showing the maximum anteroposterior diameter (APD) were identified. The BPD, representing the maximum horizontal distance between the outermost points of the parietal bones, was measured on the selected slice. Similarly, the APD, which was the maximum distance from the glabella (the most prominent point on the frontal bone) to the opisthocranion (the most posterior point of the occipital bone), was measured (►Fig. 5).
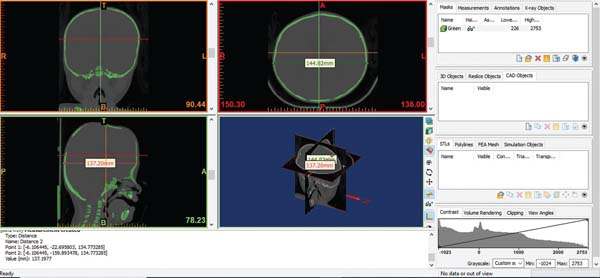

The CI was then calculated using the formula: CI = (BPD / APD) × 100, with the result expressed as a percentage. The index was used to categorize cranial shapes as dolichocephalic (CI < 75%), mesocephalic (CI: 75–80%), or brachycephalic (CI > 80%).
Statistical Analysis
Data entry and descriptive analysis were performed using the IBM SPSS Statistics for Windows (IBM Corp.), version 27.0. Numerical data were presented as mean ± standard deviation (SD) for normally distributed variables or median and interquartile range (IQR) for non-normally distributed variables. Categorical data were summarized as frequency and percentage.
Normality was assessed using the Shapiro-Wilk test. The results indicated that postoperative ACV, as well as pre-and postoperative ACVAI and CI did not significantly deviate from normality (p > 0.05), suggesting these variables were ap-proximately normally distributed. However, preoperative ACV was not normally distributed (p < 0.05).
Given the normality results, the comparison of pre-and postoperative ACV was conducted using the Wilcoxon signed-rank test, while the comparison of pre-and postoperative ACVAI was analyzed using a paired t-test. Changes in head shape pre-and postoperatively were assessed through the McNemar test. A significance level of p ≤ 0.05 was considered statistically relevant for all tests.
Results
Over the course of the study period, 20 patients underwent FOA with and without cranial vault remodeling as a primary treatment of craniosynostosis. Of the 20 patients, one was excluded due to the unavailability of a digital preoperative CT. The study cohort consisted of 19 patients with a nearly equal gender distribution, comprising 9 males and 10 females. Most participants were of Malay ethnicity (n = 15), followed by Indian (n = 2) and Chinese (n = 1).
Multi suture craniosynostosis was the predominant presentation, observed in 17 patients (89.4%), while single-suture involvement was identified in only 2 cases (10.6%). Additionally, 13 patients (68.4%) were diagnosed with syn-dromic craniosynostosis, whereas 6 patients (31.6%) pre-sented with nonsyndromic forms. The median age at which the FOA was performed was 29 months with an IQR of 15 to 36 months. The mean surgical advancement distance was 1.58 cm, with an SD of 0.45 cm (►Table 1).
| Variable | n (%) |
|---|---|
| Sex | |
| Male | 9(47.4) |
| Female | 10 (52.6) |
| Ethnicity | |
| Malay | 15 (78.9) |
| Chinese | 1 (5.3) |
| Indian | 2 (10.5) |
| Number of sutures | |
| Single | 2 (10.6) |
| Multisuture | 17 (89.4) |
| Syndromic | |
| No | 6(31.6) |
| Yes | 13 (68.4) |
| Variable | Median (IQR); Mean (SD) |
| Age at FOA (months) | 29 (15-36) |
| Distance of FOA (cm) | 1.58 (0.45) |
Abbreviations: FOA, fronto-orbital advancement; IQR, interquartile range; SD, standard deviation.

Preoperatively, the mean ACV was 259.15 cm3 (SD: 162.61 cm3). Postoperatively, ACV increased to 314.38 cm3 (SD: 79.78 cm3), reflecting a statistically significant mean increase of 55.2 3cm3 (95% confidence interval: -8.13–118.59, p = 0.042), as shown in ►Tables 2 and 3. Similarly, the ACVAI had a preoperative mean value of 1.14 (SD: 4.78), which changed to -1.63 (SD: 4.98) postoperatively, with a mean difference of 2.76 (95% confidence interval: -0.64– 6.17, p = 0.05), indicating significant improved cranial symmetry (►Tables 2 and 3).
| Variable | Mean (SD) |
|---|---|
| Preoperative | |
| ACV | 259.15 (162.61) |
| ACVAI | 1.14 (4.78) |
| Postoperative | |
| ACV | 314.38 (79.78) |
| ACVAI | -1.63 (4.98) |
Abbreviations: ACV, anterior cranial volume; ACVAI, anterior cranial vault asymmetry index; SD, standard deviation.

| Variables | Preoperative Mean (SD) | Postoperative Mean (SD) | Mean difference (95% CI) | p-value* |
|---|---|---|---|---|
| ACV | 259.15 (162.60) | 314.38 (79.78) | 55.23 (-8.13-118.59) | 0.042 |
| ACVAI | 1.14 (4.77) | -1.6 (4.98) | 2.76 (-0.64-6.17) | 0.05 |
Abbreviations: ACV, anterior cranial volume; ACVAI, anterior cranial vault asymmetry index; CI, confidence interval; SD, standard deviation.
* Note: Paired T test, significant at p < 0.05.

In terms of head shape classification, preoperative assessment showed that 2 patients were mesocephalic and 17 were brachycephalic. Postoperatively, their classifications remained unchanged, as analyzed using McNemar’s test (►Table 4). Despite significant volumetric and symmetry improvements, the overall head shape classification remained stable postoperatively.
| Variables | Postoperative head shape | Total* | ||
|---|---|---|---|---|
| Mesocephalic | Brachycephalic | |||
| Preoperative head shape | Mesocephalic | 2 | 0 | 2 |
| Brachycephalic | 0 | 17 | 17 | |
* Note: McNemar test.

Discussion
Surgical intervention of craniosynostosis aims to correct the shape of the head and to increase intracranial volume to allow for unrestricted brain growth. Thus, it is imperative that intervention needs to be done before there is permanent damage to the child’s brain and its function. The ideal timing of surgery occurs before the age of 1-year-old, when the brain undergoes maximal growth. This helps to provide internal molding force postoperatively and when the skull bones are still malleable enough for reshaping and fixation.2,15,17
One of the main surgical interventionS for craniosynostosis is FOA, especially in cases with premature closure involving either the metopic or coronal sutures.6–12 It can be done in isolation or with cranial vault remodeling, assisting in the anterior expansion of the cranial vault, which enables correction of the deformities and asymmetries to the frontal region.
Achieving a symmetrical fronto-orbital symmetry is key to an aesthetically pleasing outcome of the FOA. However, there is a tendency for relapse to occur with more severe craniosynostosis.18 Longer follow-ups with a minimum of 1 year have shown 55 to 75% of cases after FOA showed relapse of temporal hollowing and supraorbital retrusion.12 Cephalometric analyses prove there is limited growth potential in the anterior cranial base in cases of syndromic brachycephaly.7
The use of nonabsorbable sutures as a fixation method in craniosynostosis surgery offers significant economic advantages, making it the preferred choice in our practice. In Malaysia, the costs of these sutures are fully covered by the government, ensuring universal access without financial burden. In contrast, resorbable plates are not subsidized, requiring patients to bear the full cost, thereby limiting accessibility to those who can afford them, despite their clinical benefits. As such, it is crucial to evaluate the clinical outcomes of FOA using this less rigid fixation method and to assess its impact on the anterior cranial fossa.
There are several measures used to evaluate the surgical outcome of the FOA which has migrated from subjective evaluations to more objective methods. Many studies have analyzed the surgical outcome using anthropometric measurements,8,11 and/or photographs for the inclusion of postoperative outcomes into various Whitaker classifications.9,12,16 However, this classification has low interrater reliability,19 which increased the preference for more objective evaluations using 3D CT scans of intracranial volume measurement20,21 and CVAI,22 as well as 3D photometry.21 Other methods of analyzing the functional outcome of FOA evaluate resolution of symptoms caused by increased intracranial pressure and ophthalmologic dysmorphology.1,3,4,23,24
Our study population was operated on at a median age of 29 months, which is similar to the mean age of similar interventions done in the country since 2011.16 The difference in surgical timing in this country can be attributed to the awareness of this rare condition leading to delayed presentation of patients to tertiary centers. Not only that, there are few centers that offer surgical intervention of craniosynostosis in the country, as it requires a multidisciplinary team trained in craniofacial surgeries, along the support of an anesthetic team trained in managing major pediatric surgeries and syndromic patients, who often have unique airway, cardiac, and metabolic challenges.
With the majority of our study population being syndromic patients, they may also have other conditions that require optimization and intervention before undergoing FOA, especially if symptoms of raised intracranial pressure are not yet evident.
Increase in Anterior Cranial Volume (ACV)
The first objective of this study was to assess the increase in ACV following FOA using the less rigid fixation with nonabsorbable suture nylon 2/0. The results indicate a statistically significant increase in ACV from a mean preoperative volume of 259.15 (SD: 162.61) to 314.38 (SD: 79.78) cm3 postoperatively, with a mean difference of 55.23 cm3 (p = 0.042).
This volumetric expansion aligns with previous studies that have reported the effectiveness of FOA in increasing cranial volume, thereby reducing intracranial pressure and allowing for improved cranial growth. The wide confidence interval observed in this study (-8.13–118.59) suggests some variability in the degree of volume increase among patients, potentially influenced by factors such as age at surgery, severity of craniosynostosis, and underlying syndrome.
Improvement in Anterior Cranial Vault Symmetry
The second objective was to evaluate the improvement in anterior cranial vault symmetry using the ACVAI. The study found that the index’s mean score significantly improved postoperatively, changing from 1.14 (SD: 4.78) preoperatively to -1.63 (SD: 4.98) postoperatively, with a mean difference of 2.76 (p = 0.05). This finding suggests that FOA not only expands cranial volume but also enhances symmetry by addressing the disproportionate growth patterns associated with craniosynostosis.
However, the confidence interval (-0.64–6.17) suggests some degree of variability, likely due to patient-specific anatomical variations of the sutures involved, the severity of preoperative asymmetry, and the extent of advancement of the bandeau performed. Similar findings were also reported by Liang et al. in their study population after bilateral FOA and anterior cranial vault release with the nondetachable free-floating bone flap.22
Head Shape Classification Changes
The third objective of this study was to assess changes in head shape using the CI before and after FOA. Preoperative assessment classified 2 patients as mesocephalic and 17 as brachycephalic. Postoperatively, all classifications remained unchanged, as confirmed by McNemar’s test. These findings suggest that although FOA effectively increases cranial volume and improves symmetry, it does not significantly alter overall head shape classification.
The limitations of FOA in modifying CI parameters are particularly evident in cases of multisutures or syndromic craniosynostosis, such as Apert or Crouzon syndromes. In such cases, posterior vault distraction is often necessary to achieve significant changes in head shape, though this procedure is not performed in our center.
One possible explanation for the unchanged head shape postoperatively is that while FOA facilitates anterior forward movement, the posterior cranial vault remains unchanged, resulting in only minimal APD alterations. Postoperative cranial dysmorphology from FOA has also been correlated with the unchanged head shape in previous studies, similar to what was observed in our study.25,26
Research suggests that more severe preoperative deformities are associated with greater postoperative asymmetry, with a risk of it reverting to the preoperative head shape.25 The degree of overcorrection can be explored to achieve better postoperative results, specifically in combination with posterior vault expansion and subsequent release, which can help achieve a change in head shape.27
Limitations and Future Research
Despite the significant increase in anterior cranial volume and improved symmetry observed postoperatively, the long-term outcomes remain uncertain due to the study’s short duration. To address this gap, we recommend further research following the study population until maximum head growth is achieved.
Moreover, to minimize patient loss to follow-up in long-term studies, it is essential to establish a national craniosynostosis registry. Such a registry would not only improve patient tracking but also provide a larger sample size for future research, given the rarity of this condition.
Additionally, there is a lack of anthropometric data to determine whether the increase in ACV aligns with normal population parameters. Future studies should compare affected children with age-and sex-matched control cohorts, using similar study materials and methodologies to provide more robust insights.
Conclusion
The use of FOA with less rigid fixation with nonabsorbable sutures has demonstrated significant improvements in ACV and cranial symmetry, supporting its efficacy as a cost-effective surgical technique for craniosynostosis management. However, our findings indicate that while the procedure effectively expands cranial volume, it does not significantly alter head shape classification. These results should be interpreted cautiously due to limitations, such as the small sample size and the ethnic homogeneity of our cohort. Further research is needed to confirm these findings in larger, more diverse populations and to assess long-term outcomes.
REFERENCES
1. Rafique Ali AA, Ismail F, May CM, et al. Ophthalmic features of craniosynostosis: A Malaysian experience. Eur J Ophthalmol 2022;32(03):1417–1423. Doi: 10.1177/11206721211030093
2. Forrest C, Riesel J, Shakir S, Taylor J, Hopper R, Massenburg B. Volume Three: Craniofacial, Head and Neck Surgery and Pediatric Surgery. In: Losee J, Neligan P, Hopper R, Liu D (eds). Plastic Surgery. 5th ed. Philadelphia: Elsevier; 2024:775–854
3. Yu JW, Xu W,Wink JD,Wes AM, Bartlett SP, Taylor JA. Strabismus in Unicoronal Craniosynostosis: Effect of Orbital Dysmorphology and Fronto-Orbital Advancement and Remodeling. Plast Reconstr Surg 2020;145(02):382e–390e. Doi: 10.1097/PRS.0000000000006479
4. Lee SJ, Dondey J, Greensmith A, Holmes AD, Meara JG. The effect of fronto-orbital advancement on strabismus in children with unicoronal synostosis. Ann Plast Surg 2008;61(02):178–180. Doi: 10.1097/SAP.0b013e31815a355c
5. Hariri F, Farhana NA, Abdullah NA, et al. Optic canal characteristics in pediatric syndromic craniosynostosis. J Craniomaxillofac Surg 2021;49(12):1175–1181. Doi: 10.1016/j.jcms.2021.06.017
6. Yang B, Ni J, Li B. 3D morphological change of skull base and fronto-temporal soft-tissue in the patients with unicoronal craniosynostosis after fronto-orbital advancement. Childs Nerv Syst 2018;34(05):947–955. Doi: 10.1007/s00381-018-3721-1
7. Reinhart E, Mühling J, Michel C, Collmann H, Pistner H, Reuther J. Craniofacial growth characteristics after bilateral fronto-orbital advancement in children with premature craniosynostosis. Childs Nerv Syst 1996;12(11):690–694. Doi: 10.1007/BF00366152
8. Patel KB, Skolnick GB, Mulliken JB. Anthropometric Outcomes following Fronto-Orbital Advancement for Metopic Synostosis. Plast Reconstr Surg 2016;137(05):1539–1547. Doi: 10.1097/PRS.0000000000002129
9. Safi AF, Kreppel M, Grandoch A, Kauke M, Nickenig HJ, Zöller J. Clinical Evaluation of Standardized Fronto-Orbital Advancement for Correction of Isolated Trigonocephaly. J Craniofac Surg 2018;29(01):72–75. Doi: 10.1097/SCS.0000000000004058
10. Kampf S, Micko A, Schwartz E, Schopper C, Reinprecht A. Clinical and aesthetic outcome analysis of a case series of trigonocephaly patients after early fronto-orbital advancement. Int J Oral Maxillofac Implants 2020;49(09):1115–1121. Doi: 10.1016/j.ijom.2020.02.017
11. Metzler P, Zemann W, Jacobsen C, Grätz KW, Obwegeser JA. Cranial vault growth patterns of plagiocephaly and trigonocephaly patients following fronto-orbital advancement: a long-term anthropometric outcome assessment. J Craniomaxillofac Surg 2013;41(06):e98–e103. Doi: 10.1016/j.jcms.2012.11.035
12. Taylor JA, Paliga JT, Wes AM, et al. A critical evaluation of longterm aesthetic outcomes of fronto-orbital advancement and cranial vault remodeling in nonsyndromic unicoronal craniosynostosis. Plast Reconstr Surg 2015;135(01):220–231. Doi: 10.1097/PRS.0000000000000829
13. Fearon JA. Rigid fixation of the calvaria in craniosynostosis without using “rigid” fixation. Plast Reconstr Surg 2003;111(01):27–38, discussion 39. Doi: 10.1097/01.PRS.0000036261.99248.09
14. Linz C, Kunz F, Krauß J, et al. Stable fixation with absorbable sutures in craniofacial surgery. J Craniomaxillofac Surg 2016;44(05):622–625. Doi: 10.1016/j.jcms.2016.02.006
15. Kovács AF, Sauer SN, Stefenelli U, Klein C. Growth of the orbit after frontoorbital advancement using nonrigid suture vs rigid plate fixation technique. J Pediatr Surg 2008;43(11):2075–2081. Doi: 10.1016/j.jpedsurg.2008.03.057
16. Koh KL, Zain A. Surgical outcome after less “rigid” fixation in open cranial vault remodeling for craniosynostosis. J Craniofac Surg 2018;29(04):861–867. Doi: 10.1097/SCS.0000000000004347
17. Marchac D, Renier D, Broumand S. Timing of treatment for craniosynostosis and faciocraniosynostosis: a 20-year experience. Br J Plast Surg 1994;47(04):211–222. Doi: 10.1016/0007-1226(94)90001-9
18. Lwin CTTJW, Richardson D, Duncan C, May P. Relapse in frontoorbital advancement: a pilot study. J Craniofac Surg 2011;22(01):214–216. Doi: 10.1097/SCS.0b013e3181f76081
19. Wes AM, Naran S, Sun J, et al. The Whitaker classification of craniosynostosis outcomes: An assessment of interrater reliability. Plast Reconstr Surg 2017;140(04):579e–586e. Doi: 10.1097/PRS.0000000000003688
20. Sulong S, Alias A, Johanabas F, Abdullah JY, Idris B. Intracranial Volume Post Cranial Expansion Surgery Using Three-Dimensional Computed Tomography Scan Imaging in Children With Craniosynostosis. J Craniofac Surg 2020;31(01):46–50. Doi: 10.1097/SCS.0000000000005810
21. Freudlsperger C, Steinmacher S, Bächli H, Somlo E, Hoffmann J, Engel M. Metopic synostosis: Measuring intracranial volume change following fronto-orbital advancement using three-dimensional photogrammetry. J Craniomaxillofac Surg 2015;43(05):593–598. Doi: 10.1016/j.jcms.2015.02.017
22. Liang QC, Chen X, Yang B, et al. Bilateral fronto-orbital advancement combined with cranial vault release using a free-floating bone flap technique for nonsyndromic unilateral coronal synostosis. Transl Pediatr 2023;12(12):2213–2221. Doi: 10.21037/tp-23-495
23. Shi L, Shen W, Gao Q, Kong L. The PostoperativeMorphometrics of Orbital and Maxillary Area for Craniosynostosis. J Craniofac Surg 2019;30(07):2091–2093. Doi: 10.1097/SCS.0000000000005987
24. Gencarelli JR, Murphy A, Samargandi OA, Bezuhly M. Ophthalmologic outcomes following fronto-orbital advancement for unicoronal craniosynostosis. J Craniofac Surg 2016;27(07):1629–1635. Doi: 10.1097/SCS.0000000000003085
25. Beiriger JW, TaoW, Irgebay Z, et al. A Longitudinal Analysis of Preand Post-Operative Dysmorphology inMetopic Craniosynostosis. Cleft Palate Craniofac J 2024;62(07):1144–1150. Doi: 10.1177/10556656241237605
26. Tio PAE, Abdel Alim T, Roshchupkin G, et al. Forehead shape analysis following surgical and conservative treatment in metopic synostosis: a 3D photogrammetry analysis. Plast Reconstr Surg 2024;156(01):103e–111e. Doi: 10.1097/PRS.0000000000011753
27. Choi M, Flores RL, Havlik RJ. Volumetric analysis of anterior versus posterior cranial vault expansion in patients with syndromic craniosynostosis. J Craniofac Surg 2012;23(02):455–458. Doi: 10.1097/SCS.0b013e318240ff49
1. Reconstructive Sciences Unit, School of Medical Sciences, Universiti Sains Malaysia,
Kota Bahru, Kelantan, Malaysia
2. Department of Plastic and Reconstructive Surgery Department, Hospital Kuala Lumpur,
Jalan Pahang, Kuala Lumpur, Malaysia
3. Departamento de Radiologia, Hospital Tunku Azizah, Jalan Raja Muda Abdul Aziz,
Kampung Baru, Kuala Lumpur, Malaysia
4. Craniofacial Medical Imaging Cluster Research and Innovation Unit, School of Dental
Sciences, Universiti Sains Malaysia, Kelantan, Malaysia
5. Dental Research Unit, Center for Transdisciplinary Research (CFTR), Saveetha Dental
College, Saveetha Institute of Medical and Technical Sciences, Saveetha University,
Chennai, India
Data Availability Data will be available upon request to the corresponding author.
Ethical Approval Ethical approval was obtained from the Malaysian Medical Research and Ethics Committee [NMRR ID-2402969-TW0 (IIR)] and the Human Research Ethics Committee of Universiti Sains Malaysia [USM/JEPeM/KK/ 24080675].
Financial Support The authors declare that they did not receive financial support from agencies in the public, private or nonprofit sectors to conduct the present study.
Address for correspondence Rebecca Choy Xin Yi, Reconstructive Sciences Unit, School of Medical Sciences, Universiti Sains Malaysia, 16150, Kota Bahru, Kelantan, Malaysia (e-mail: rebecca.tusc@gmail.com).
Article received: May 24, 2025.
Article accepted: August 12, 2025.
Conflict of Interests The authors have no conflict of interests to declare.
Editor-in-Chief: Dov Charles Goldenberg.
 Read in Portuguese
Read in Portuguese
 Read in English
Read in English
 PDF PT
PDF PT
 Print
Print
 Send this article by email
Send this article by email
 How to Cite
How to Cite
 Mendeley
Mendeley
 Pocket
Pocket